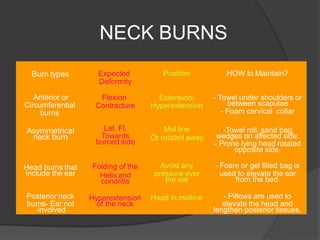
This document discusses problems associated with managing patients with post-burn contractures of the neck. It notes risks like restricted neck and airway, difficulty with intubation, malnutrition and anemia. Relevant history, examinations, investigations, patient preparation, anesthesia considerations and post-op care are outlined. Surgical release of contractures and skin grafting/flaps are described as treatment, along with physiotherapy and pressure garments. Challenges include repeated surgery, positioning, psychological issues and prolonged hospital stay.