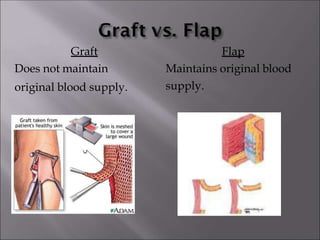
1. The document discusses skin grafts, defining grafts as tissue detached from its blood supply and placed in a new area, while flaps retain some original blood supply.
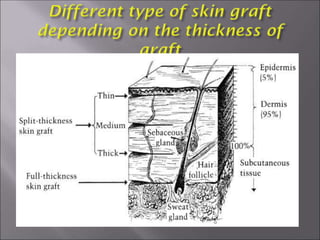
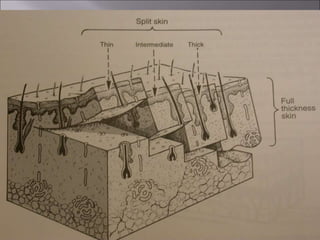
2. It classifies grafts as autografts, allografts, or xenografts based on donor species, and as thin, thick, or full thickness based on depth.
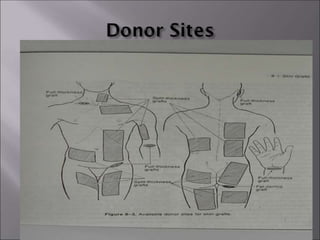
3. The ideal donor site provides skin identical to the recipient area, but skin varies in color, thickness, hair, and texture between body sites. Common donor sites include the post auricular area, upper eyelid, and thigh.