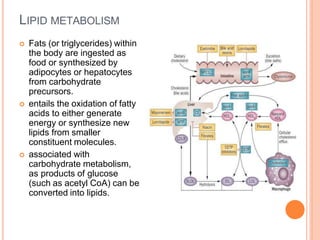
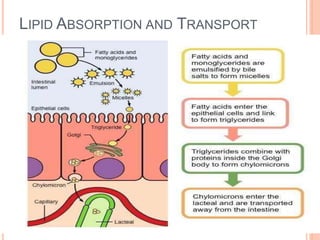
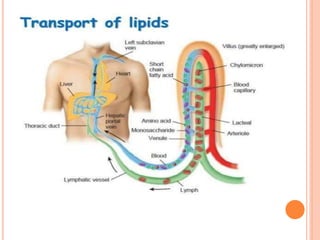
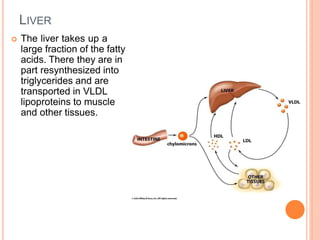
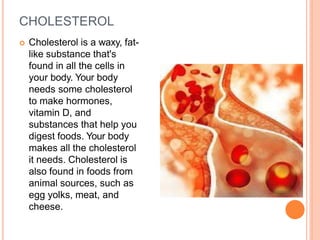
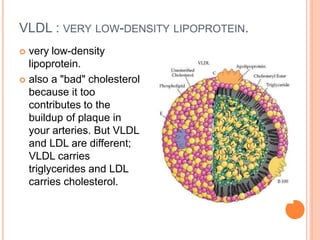
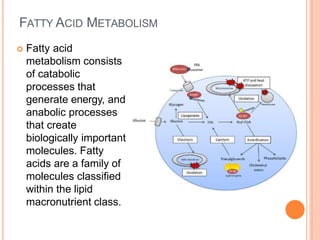
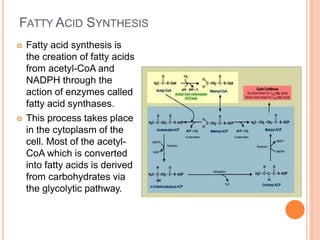
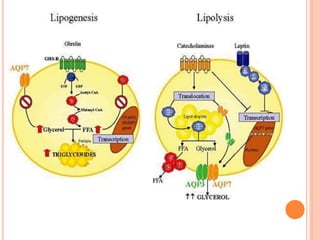
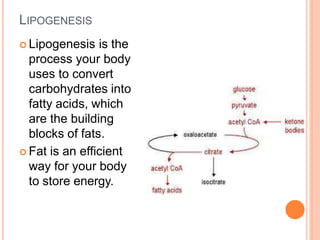
Lipid metabolism involves the breakdown of fats into fatty acids to produce energy or the synthesis of new lipids from smaller molecules. Fats can be obtained from food or synthesized in the liver or adipose tissue. Lipids are stored as triglycerides in adipose tissue and mobilized for energy through lipolysis. The liver plays a key role in lipid metabolism by breaking down fats and producing energy, cholesterol, and phospholipids. Lipids are essential for many bodily functions when consumed in proper amounts.







































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)
















