Downloaded 923 times






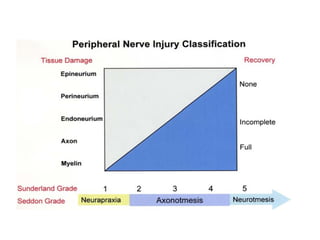
























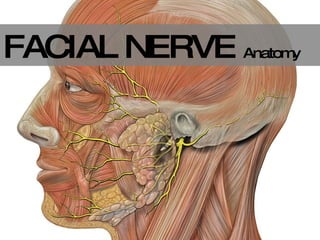








This document discusses peripheral nerve injuries, including anatomy, types of injuries (acute vs chronic), clinical signs, pathophysiology, and examples of specific nerve injuries like carpal tunnel syndrome and radial nerve palsy. Treatment options are also summarized, including conservative treatment with medications for mild cases and surgical indications like nerve repair, grafting, or release surgery for severe or failed conservative cases.























































































