Downloaded 114 times




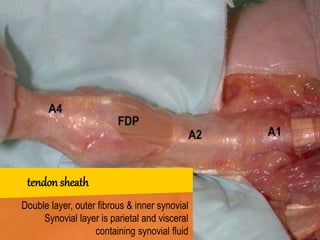
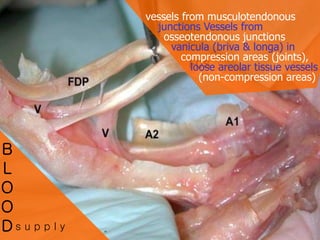
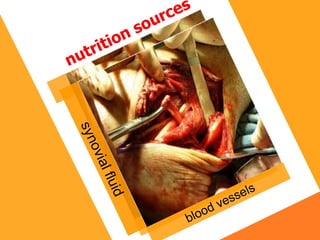
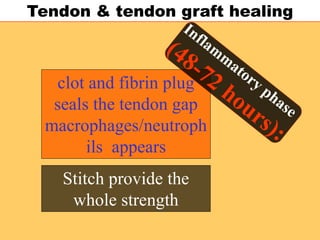




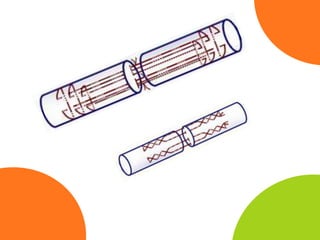
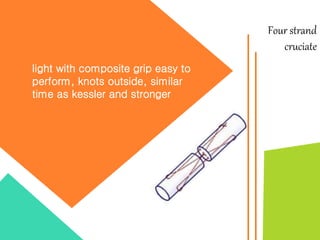

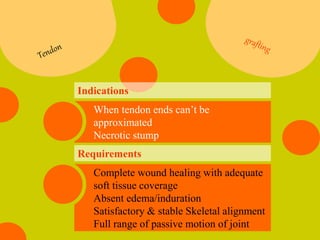









This document discusses tendon healing and repair techniques. It covers the histology of tendons, the tendon healing process, and various techniques for tendon repair including suturing methods and tendon grafting. Key points include that both intrinsic and extrinsic healing contribute to tendon repair, and techniques like controlled motion help promote healing while preventing adhesions. Suturing methods like the Kessler and cruciate repairs are discussed and compared. Tendon grafting indications and requirements are also outlined.





























































































