1. Small, superficial nasal defects less than 1.5 cm can be reconstructed with primary closure, full thickness skin grafts, or local flaps like bilobed or VY flaps depending on the location on the nose.
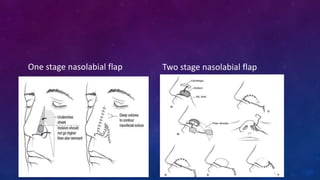
2. Larger or deeper defects requiring cartilage graft support can utilize septal or rib cartilage grafts along with regional pedicled flaps like nasolabial or forehead flaps.
3. Total or subtotal nasal reconstruction involving all three nasal layers requires a series of operations using free flap tissue transfer, forehead flaps, and cartilage grafts to replace all missing nasal tissues.