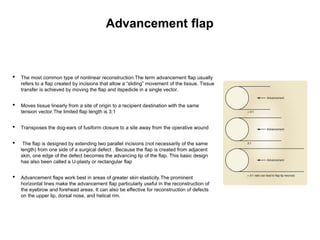
This document defines common terms used to describe flaps and their components in Mohs reconstruction. It discusses the classification of flaps and some fundamentals of flap design and suturing technique. Advancement flaps are introduced as the most common type of nonlinear reconstruction where tissue is moved in a single vector from the origin to the recipient site.