Downloaded 28 times
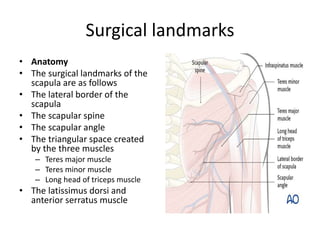
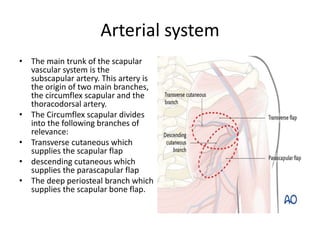
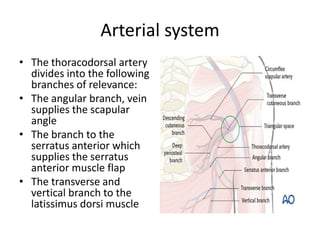
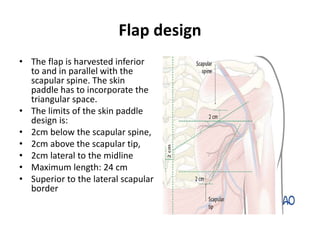
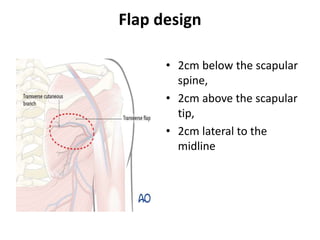
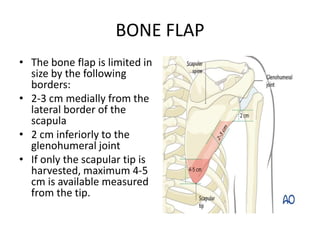
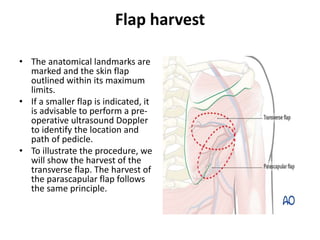
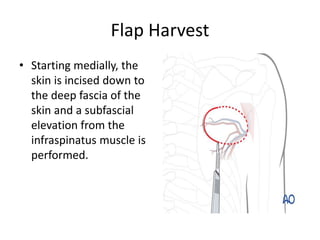
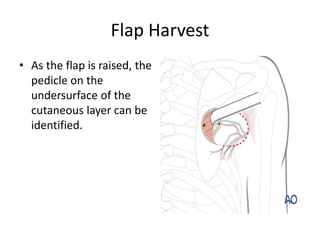
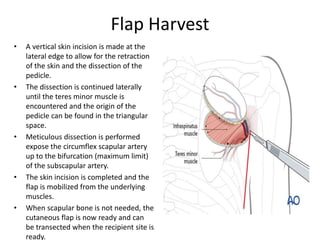
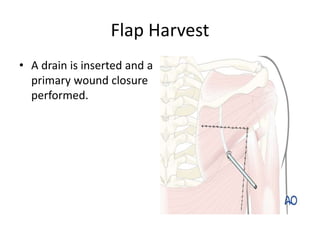
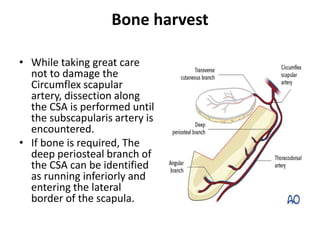
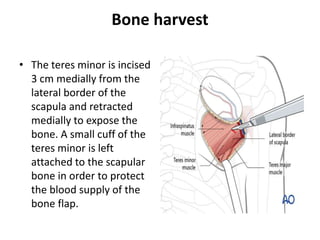
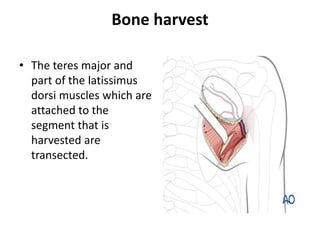
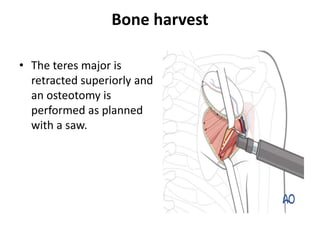
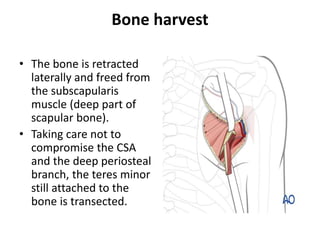
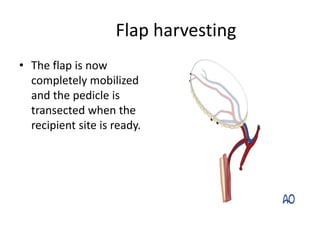

This document describes the scapular flap procedure. It details the relevant surgical landmarks and arterial system around the scapula. The flap can include skin, muscle, and bone from the scapula region. The flap is designed and harvested by following the path of the circumflex scapular artery. For a bone flap, the periosteal branch is dissected to access bone from the lateral border of the scapula. The scapular flap provides a large volume of soft tissue and bone to reconstruct significant defects, such as after extensive maxillectomies or mandibular resections.























































































