Downloaded 435 times
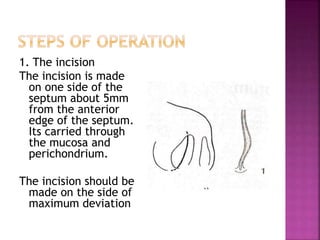
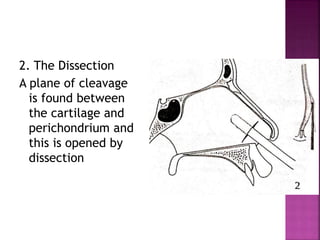
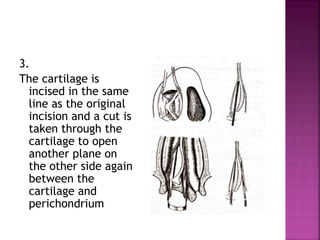
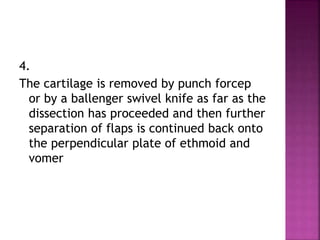




This document describes the indications, techniques, and postoperative care for septoplasty surgery. It indicates that septoplasty is performed to correct a deviated nasal septum causing obstruction or other issues. The key steps described are making an incision, raising mucoperichondrial flaps, removing deviated cartilage and bone, and re-approximating the flaps. Potential complications are also outlined.