Downloaded 80 times

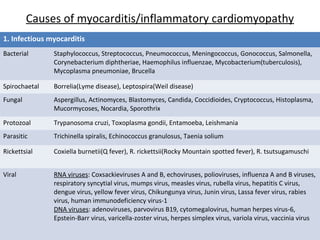
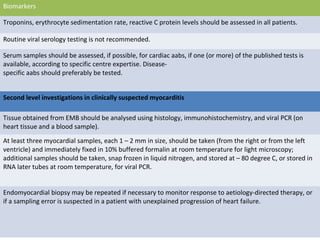

1. Myocarditis is an inflammatory disease of the myocardium diagnosed using histological, immunological and immunohistochemical criteria, with an abnormal inflammatory infiltrate defined as ≥14 leucocytes/mm including up to 4 monocytes/mm and ≥7 CD3 positive T-lymphocytes/mm. 2. Causes of myocarditis include infectious agents like viruses, bacteria, and parasites; immune-mediated reactions to drugs, vaccines or transplants; and toxic effects of drugs, heavy metals, and other toxins. 3. Diagnosis involves clinical presentations like chest pain and heart failure, as well as diagnostic criteria including ECG/imaging abnormalities, elevated cardiac biomarkers, and endomyocardial biopsy showing






























































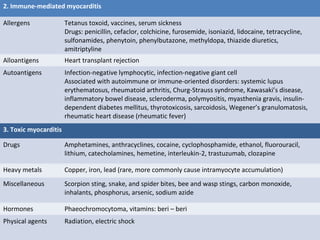
![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)










![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)






