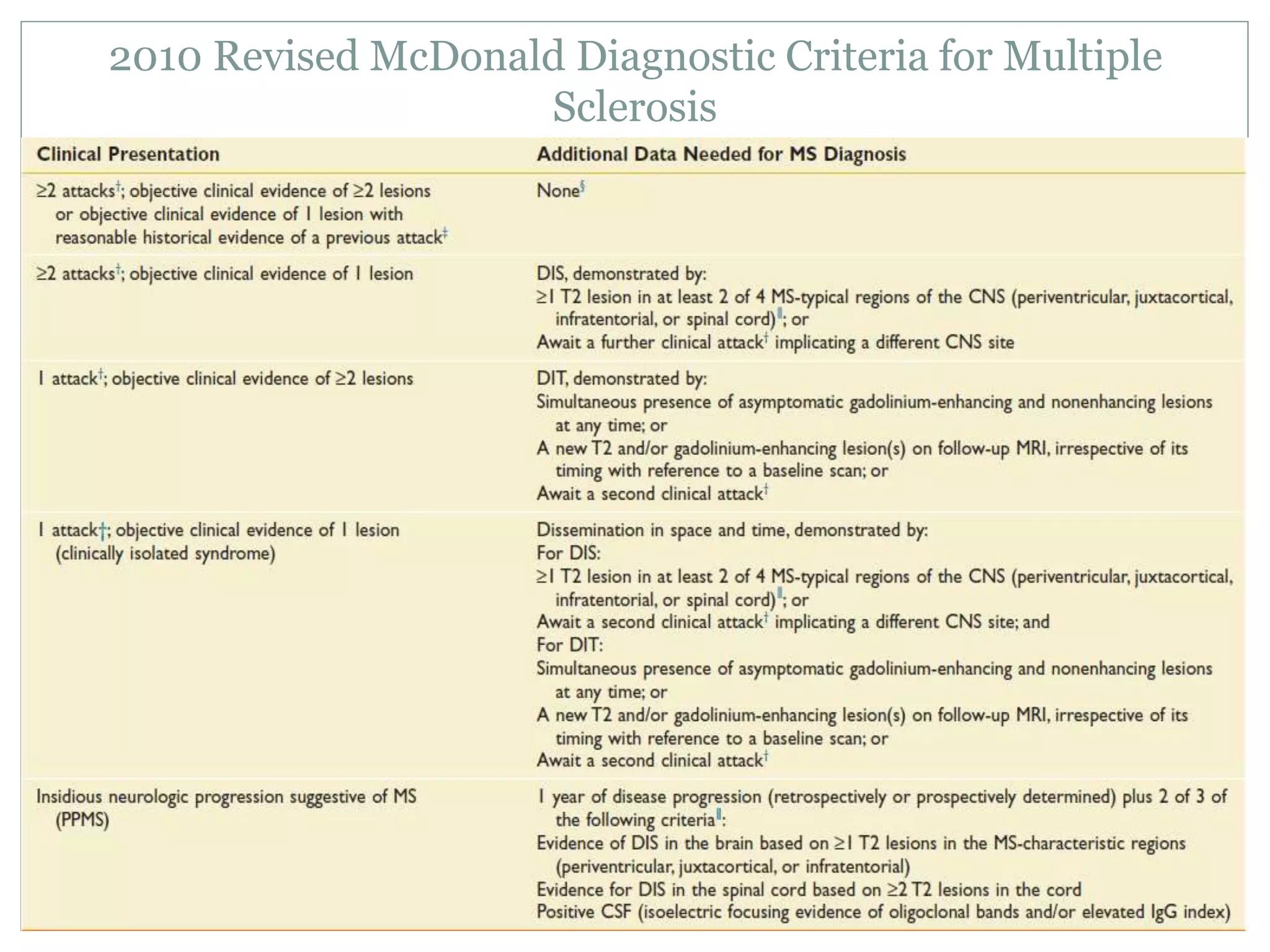
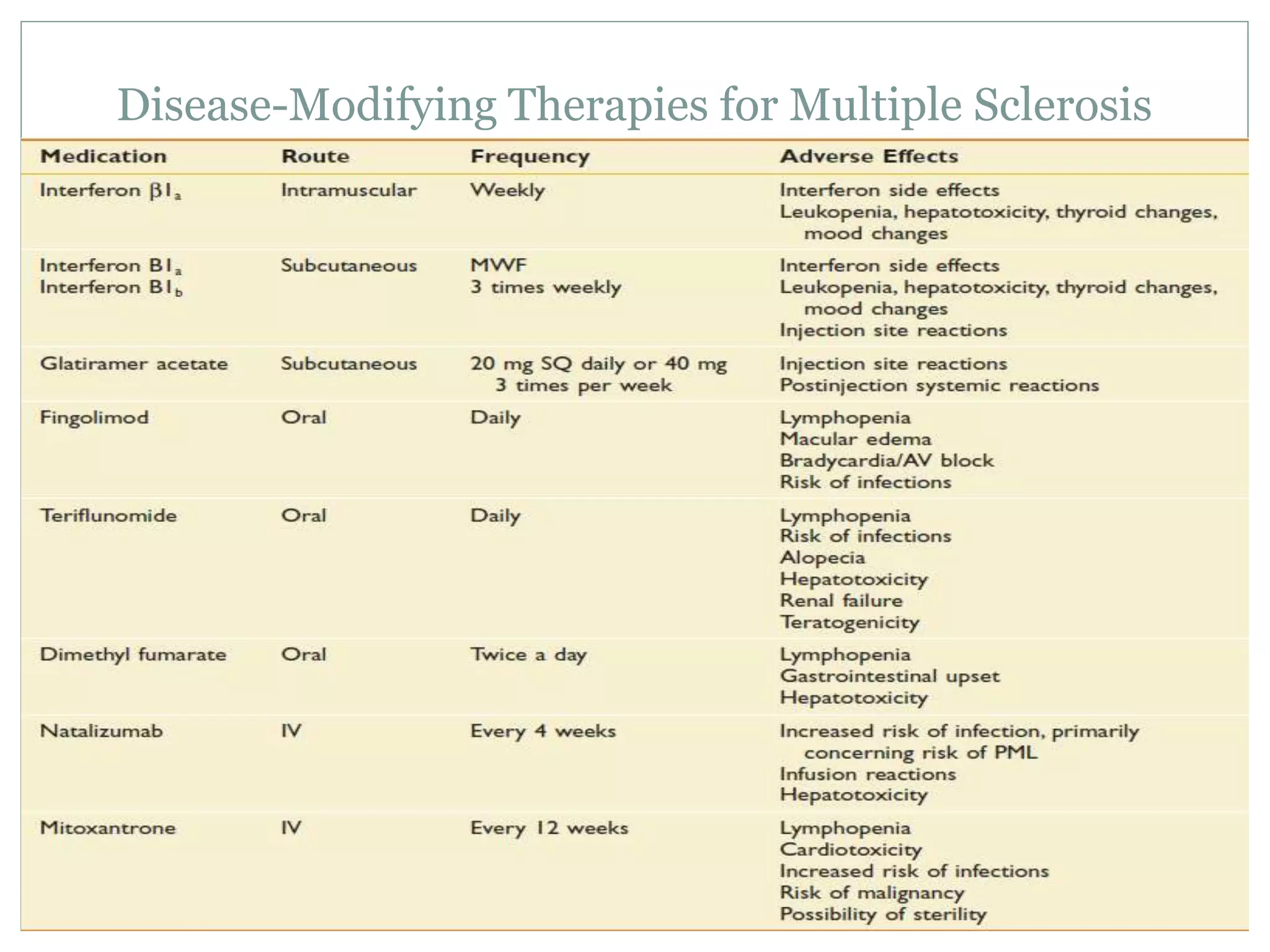
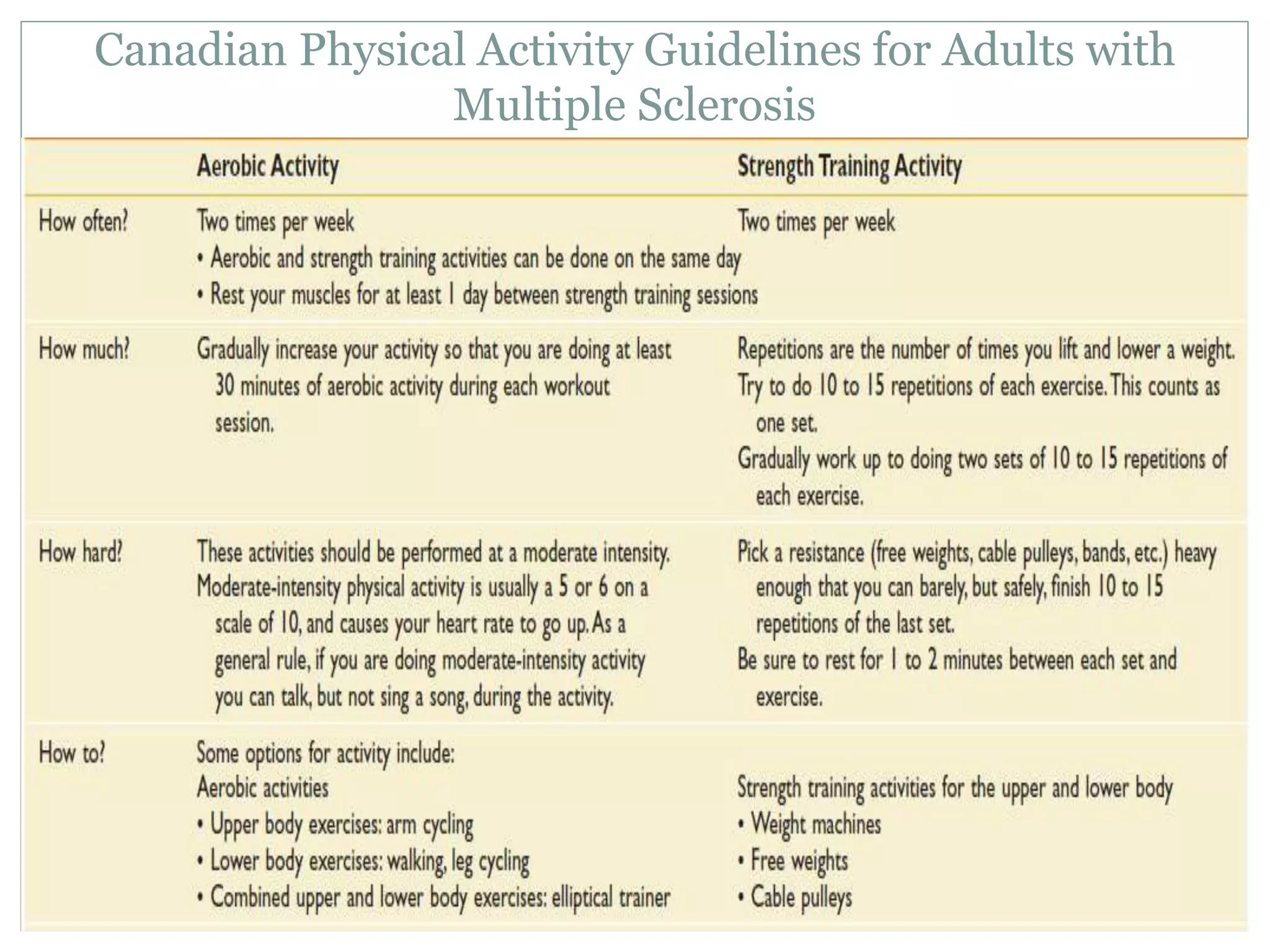
This document discusses rehabilitation principles for multiple sclerosis (MS). It begins by defining MS as a chronic, progressive disease of the central nervous system characterized by demyelination of the brain and spinal cord. It then covers the epidemiology, pathogenesis, subtypes, common symptoms and signs, diagnosis using the McDonald criteria, disease severity as measured by EDSS, disease-modifying therapies, and approaches to managing common issues like gait impairment and fatigue through rehabilitation and exercise.











































































































































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)











