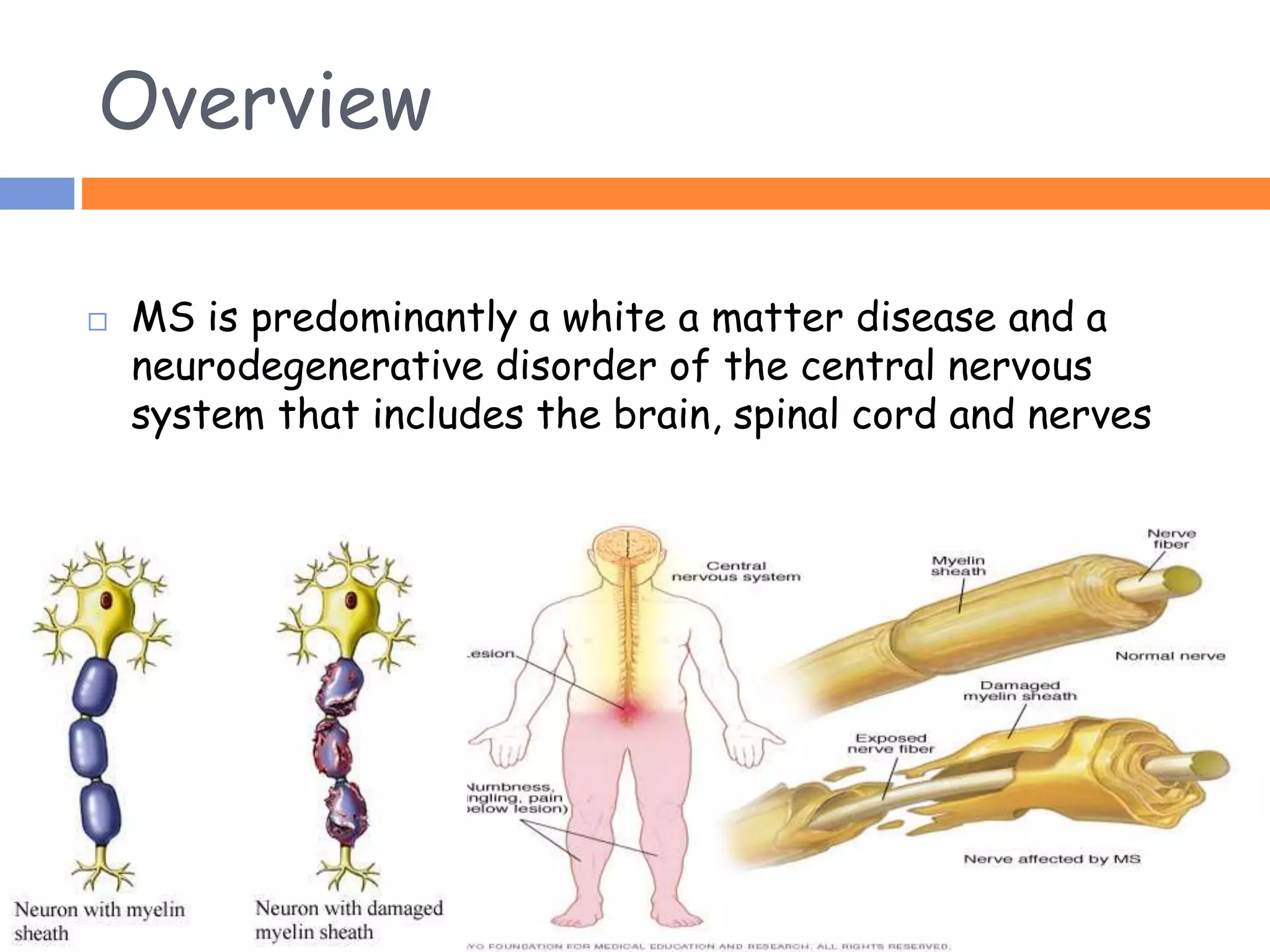
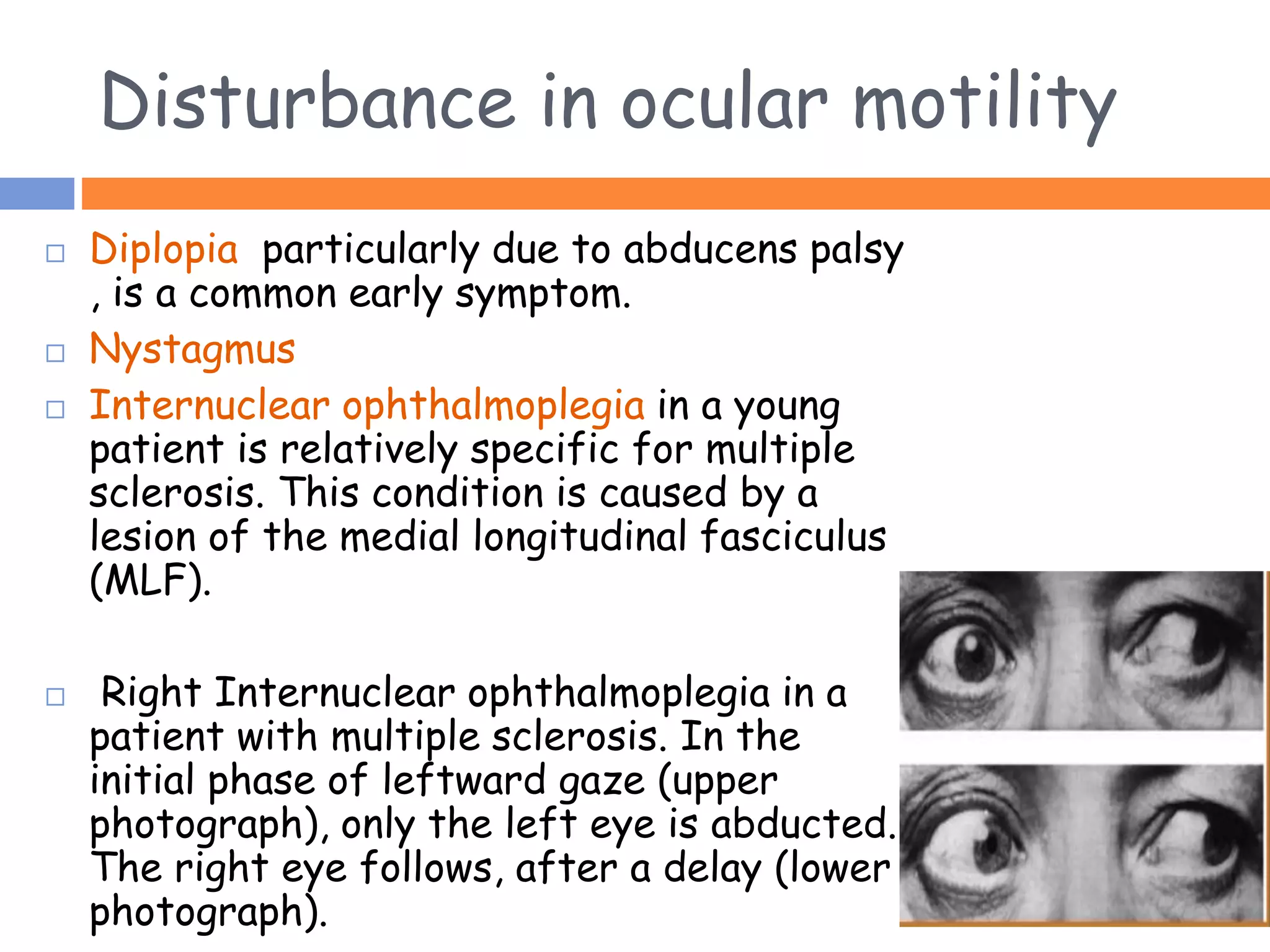
Multiple sclerosis (MS) is a neurodegenerative disease that affects the central nervous system through inflammation and demyelination. It is more common in women than men and typically occurs in young adults between 20-40 years old. MS is predominantly found in northern regions of the world. While its cause is unknown, genetic and environmental factors like infections are thought to play a role. Symptoms vary depending on the areas of the nervous system affected but can include vision problems, impaired movement, sensory issues, and mental changes. The disease progresses over time and treatment aims to manage symptoms and reduce inflammation.