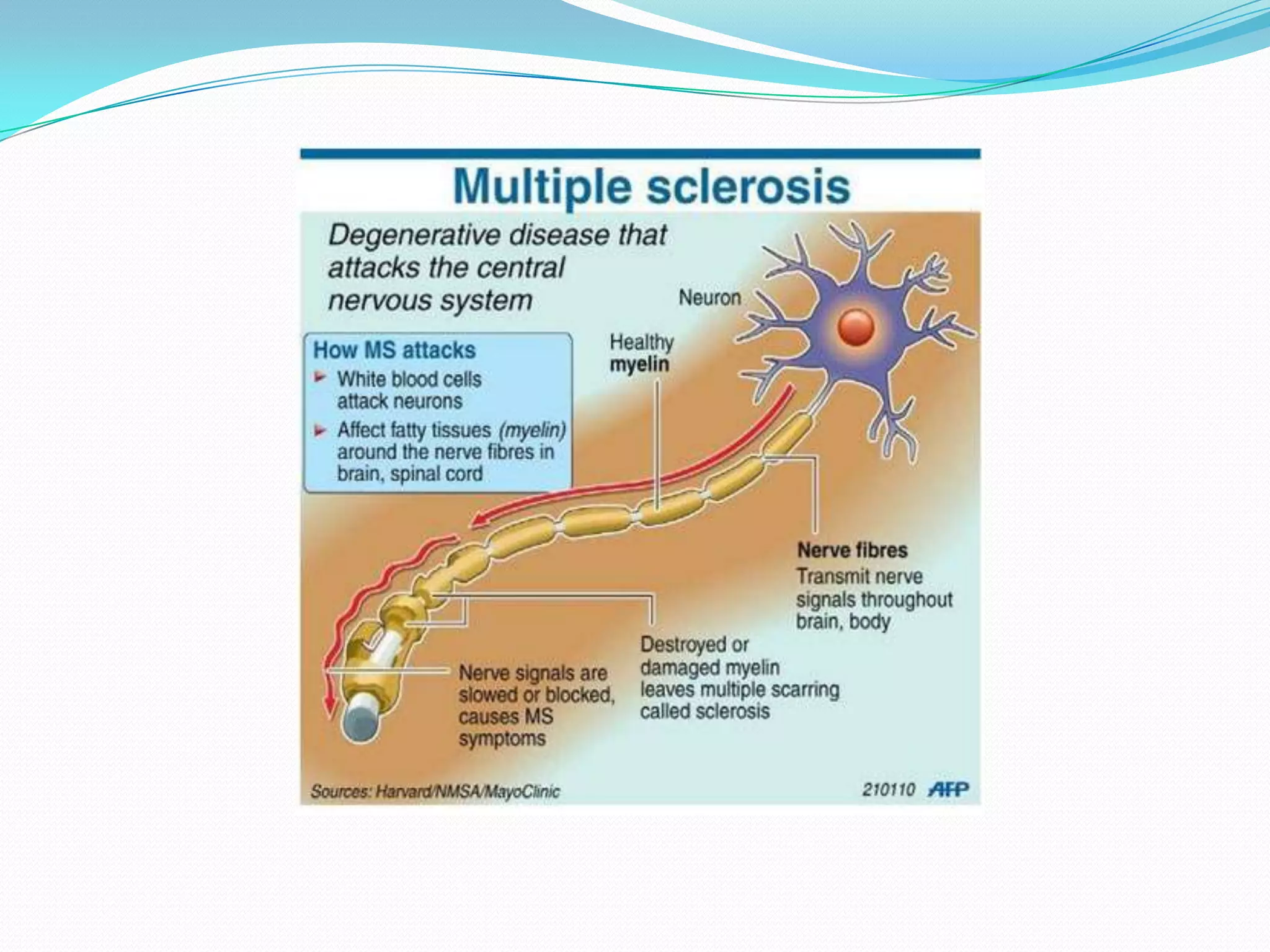
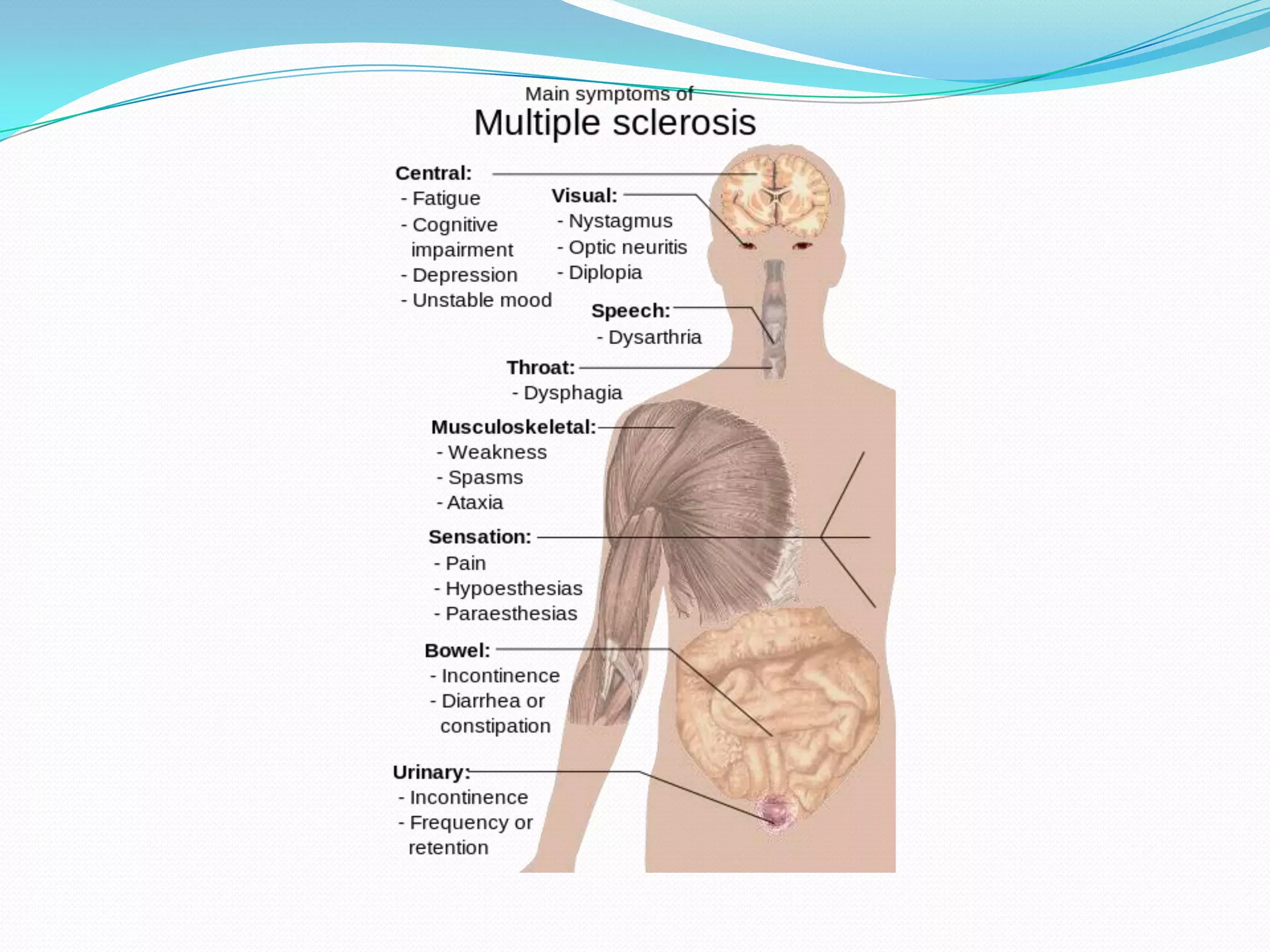
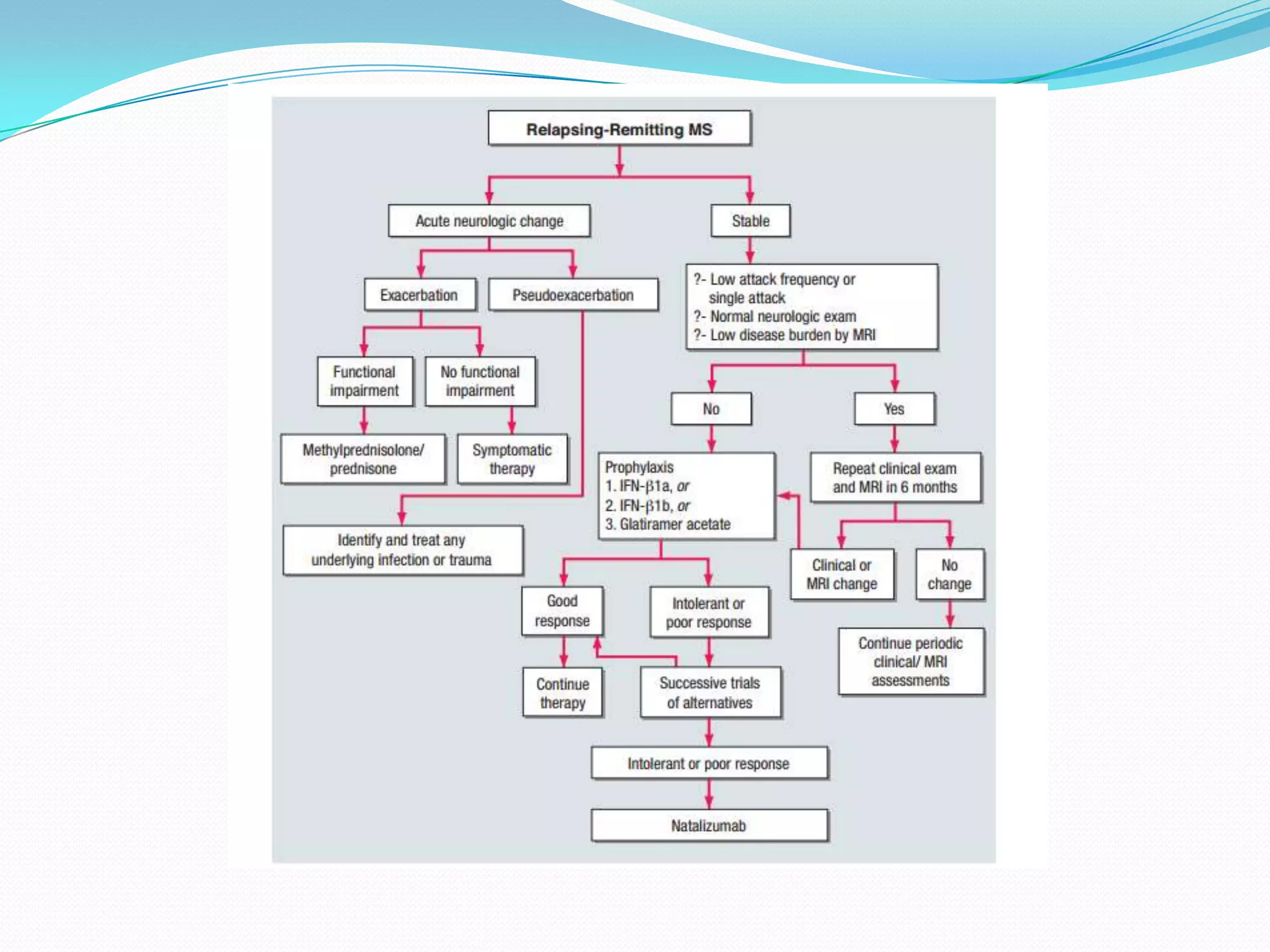
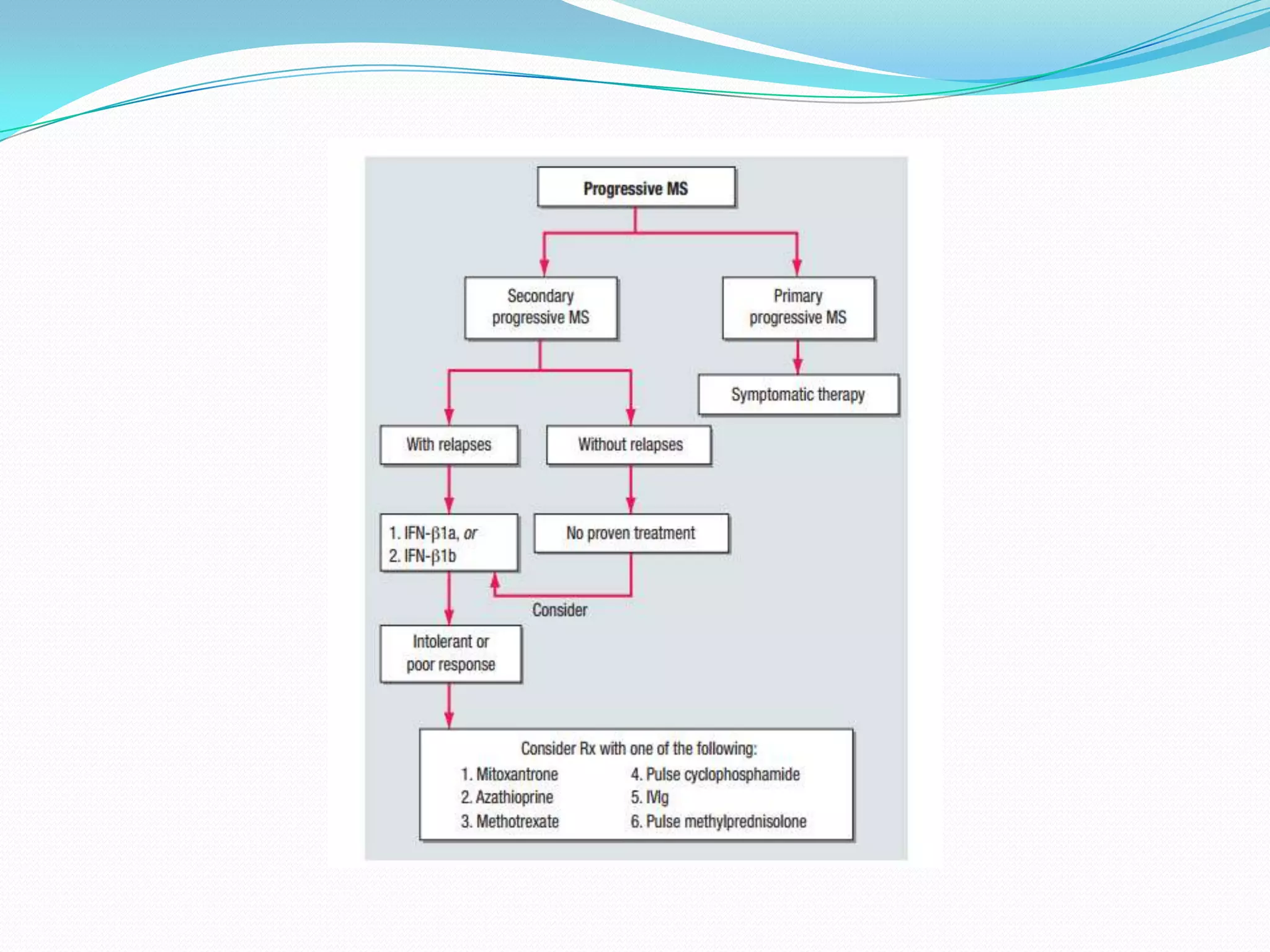
Multiple sclerosis (MS) is a demyelinating disease of the central nervous system characterized by inflammation and nerve damage. It commonly affects women under 30 years old in temperate climates. Symptoms include visual problems, numbness, weakness, and impaired coordination. While relapses may be followed by remission, over time disability accumulates without treatment. The cause is unknown but involves immune-mediated damage to myelin. Diagnosis is clinical based on dissemination of lesions in time and space. MRI is used to identify lesions. Treatment focuses on reducing relapse rate and progression with steroids, interferons, glatiramer acetate or monoclonal antibodies.