Downloaded 41 times

![• Middle East respiratory syndrome (MERS) is a respiratory disease caused by
a newly recognized coronavirus MERS-Corona virus (MERS CoV).
• It was first reported in 2012 in Saudi Arabia and is so far linked to countries
in or near the Arabian Peninsula (United Arab Emirates [UAE], Qatar,
Oman, Jordan, Kuwait, Yemen, and Lebanon).
• Till now 688 cases of MERS are reported of which 282 died , a mortality
rate of 40%.](https://image.slidesharecdn.com/mers-170215074254/85/Mers-2-320.jpg)

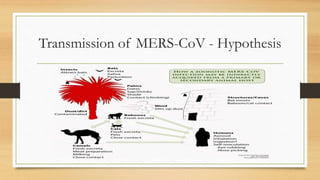

Middle East respiratory syndrome (MERS) is a respiratory disease caused by the MERS coronavirus (MERS-CoV) which was first reported in 2012 in Saudi Arabia. As of now, there have been 688 reported cases of MERS of which 282 resulted in death, a 40% mortality rate. Camels have been identified as a potential reservoir for the virus. The virus is transmitted from human to human through direct contact or contaminated surfaces and causes respiratory symptoms. There is currently no vaccine though several treatments are being investigated.
























































































