Downloaded 137 times

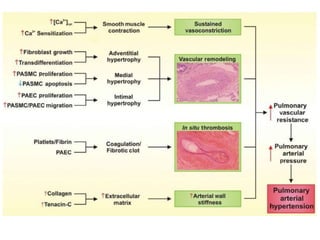
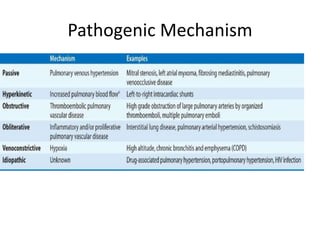
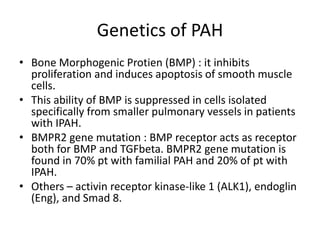

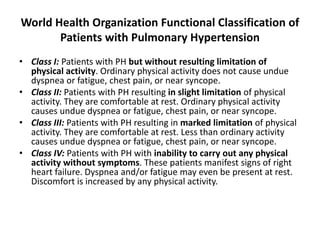
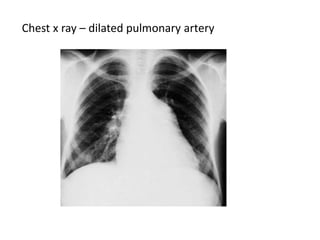
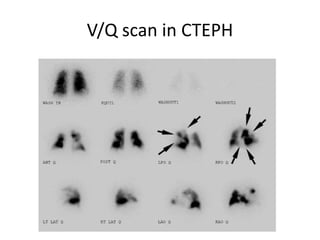
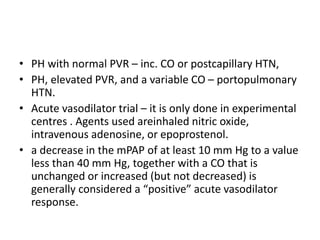
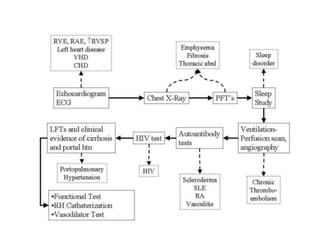
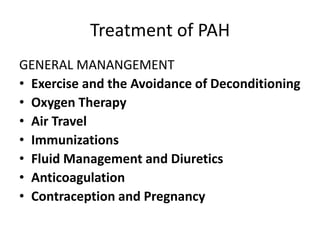
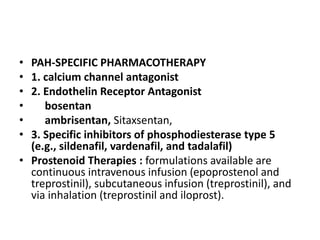



- Pulmonary artery hypertension (PAH) is defined as a mean pulmonary artery pressure of ≥25 mmHg at rest. It is characterized by pre-capillary pulmonary hypertension with a pulmonary wedge pressure <15 mmHg and a pulmonary vascular resistance >3 Wood units. - The pathophysiology involves sustained vasoconstriction, vascular remodeling, in situ thrombosis, and increased arterial stiffness. Genetic factors like BMPR2 mutations also contribute to PAH development. - Clinical features range from mild breathlessness to signs of right heart failure. Diagnostic tests include echocardiography, CT scans, V/Q scans, right heart catheterization and lab tests. - Treatment involves oxygen therapy, diure























































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)


![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)
![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)

