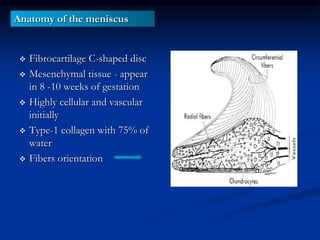
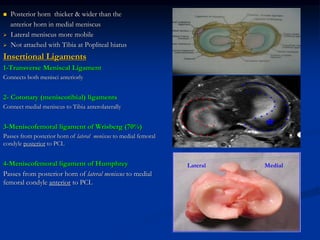
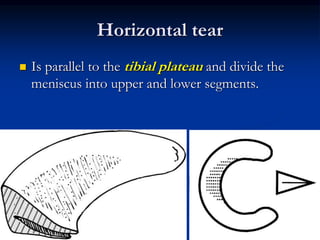
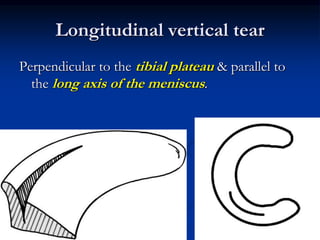
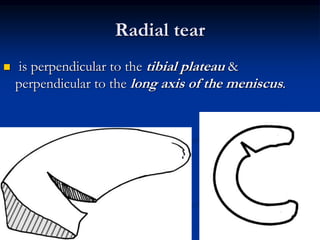
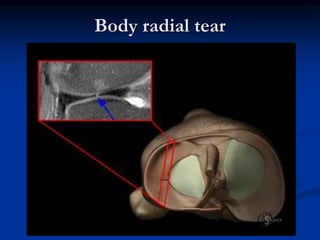
This document discusses the anatomy, biomechanics, and pathology of the meniscus in the knee. It begins by describing the structure and functions of the meniscus, including its role in load distribution, shock absorption, and joint stability. It then covers the different types of meniscal tears, categorized by their orientation (horizontal, longitudinal, radial). Imaging techniques for identifying meniscal tears are discussed, along with clinical exams. Finally, the document outlines treatment approaches, including non-surgical management and surgical options like meniscectomy, repair, and transplantation.

































































![MENISCUS 2745236382575687647634TEAR[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/meniscustear1-251213165858-d2427fa8-thumbnail.jpg?width=640&height=640&fit=bounds)





















![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)






