Downloaded 530 times
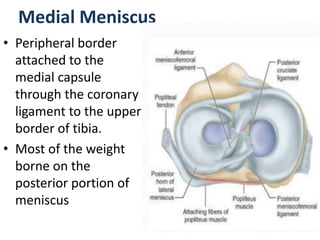
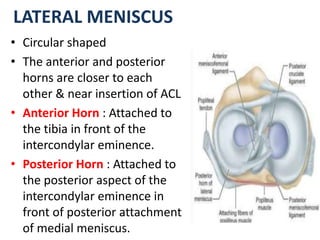
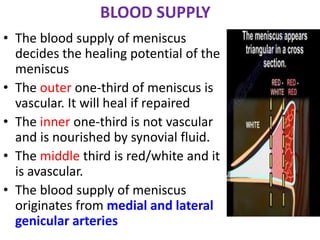
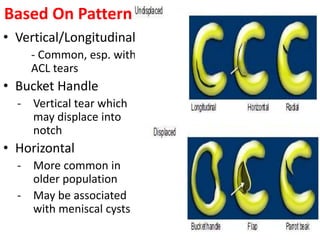

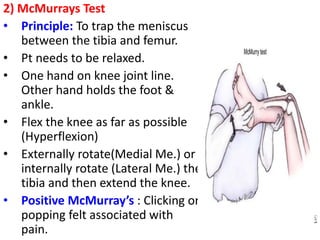
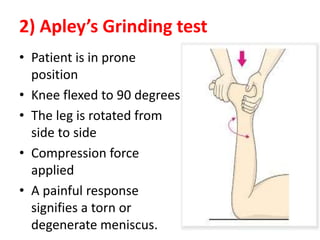

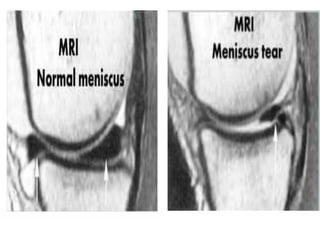

This document discusses meniscus injuries of the knee. It describes the anatomy and functions of the medial and lateral meniscus. Common types of meniscal tears are described based on location and pattern. Physical exam maneuvers for diagnosing meniscal tears include Thessaly test, McMurray's test, and Apley's grinding test. MRI is the most sensitive imaging method. Treatment involves initial rest, ice, and NSAIDs for minor tears. Surgery options include partial meniscectomy, meniscal repair, or meniscal transplantation for more severe tears. The goal of treatment is to relieve symptoms and prevent further joint damage.








































![MENISCUS 2745236382575687647634TEAR[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/meniscustear1-251213165858-d2427fa8-thumbnail.jpg?width=640&height=640&fit=bounds)







































