This document discusses the procedural guidelines and considerations for corrective osteotomy around the knee, focusing on the importance of alignment and load distribution in managing knee deformities and osteoarthritis. It outlines indications for surgery, including various deformities and post-acquired conditions, and describes surgical techniques for high tibial osteotomy, detailing the benefits and drawbacks of different approaches. Additionally, the document emphasizes the significance of proper patient selection, correction angles, and the use of specific implants for successful outcomes.



![• Post acquired epiphysiodesis [septic/traumatic]
• Congenital deformity[PFFD,NF]
• Flexion contracture in arthrogryposis,polio..
• Acquired deformity [rickets,blount disease]
• Focal chondrodysplasia.
• Post traumatic deformity..
Indication in children and
adolescent...](https://image.slidesharecdn.com/osteotomyaroundkneedrshankarjangid1-190707063819/75/Osteotomy-around-knee-dr-shankar-jangid-1-7-2048.jpg)

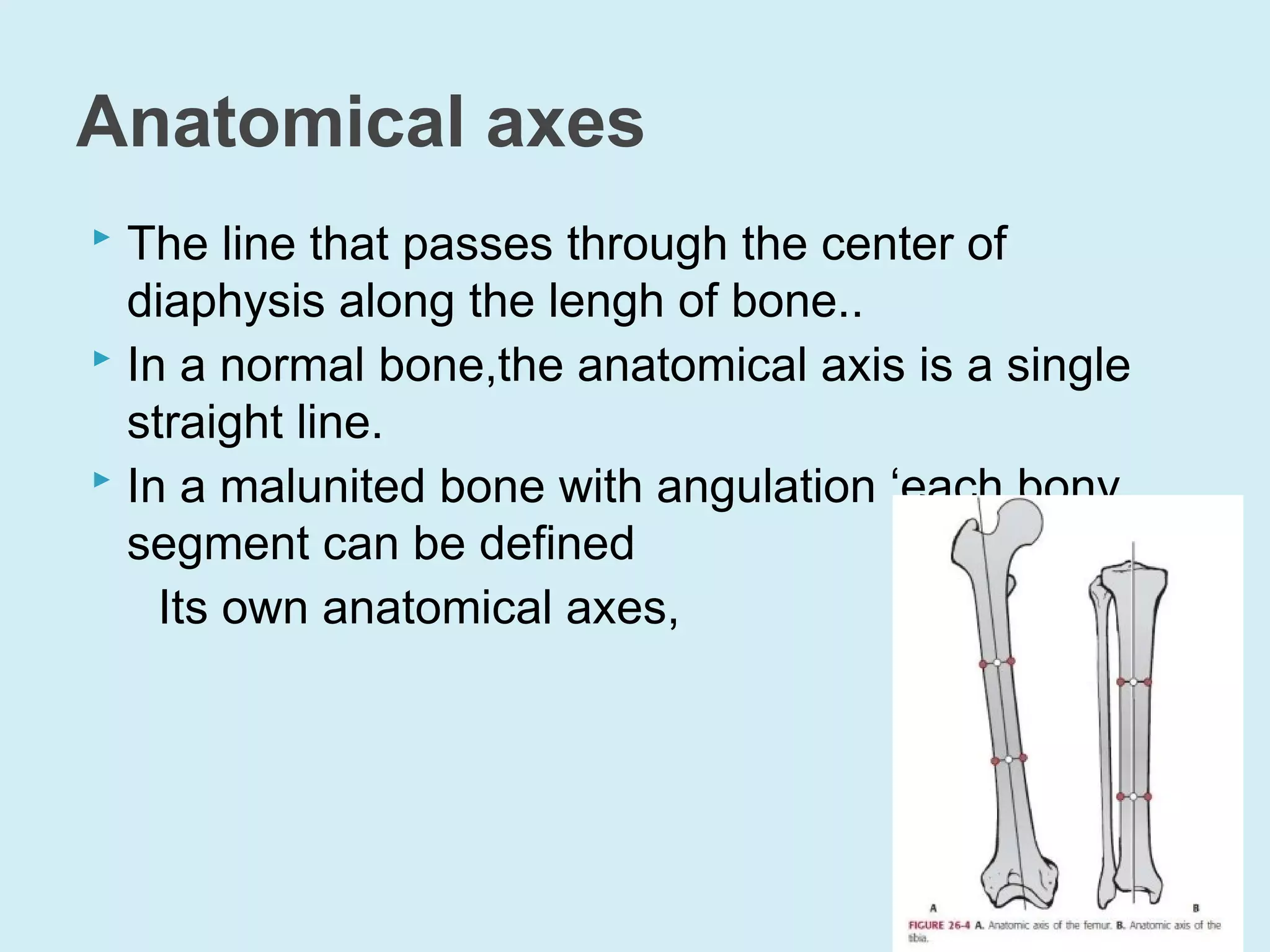
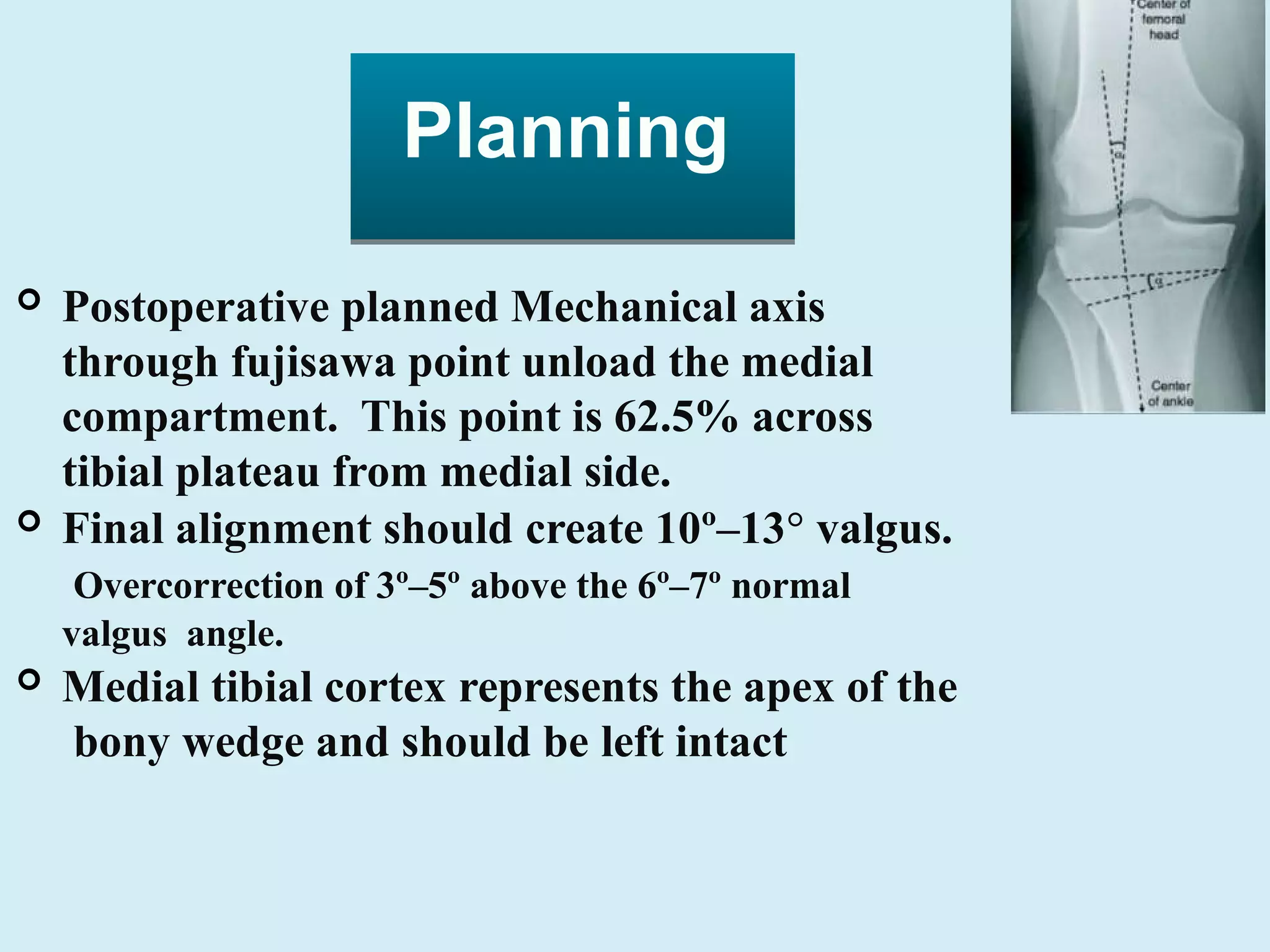
![Anatomical axis
Mechanical axis
Mechanical axis deviation
Reference Joint angle
Location of deformity[cora]
Physiological axes and joint angle of
leg](https://image.slidesharecdn.com/osteotomyaroundkneedrshankarjangid1-190707063819/75/Osteotomy-around-knee-dr-shankar-jangid-1-9-2048.jpg)



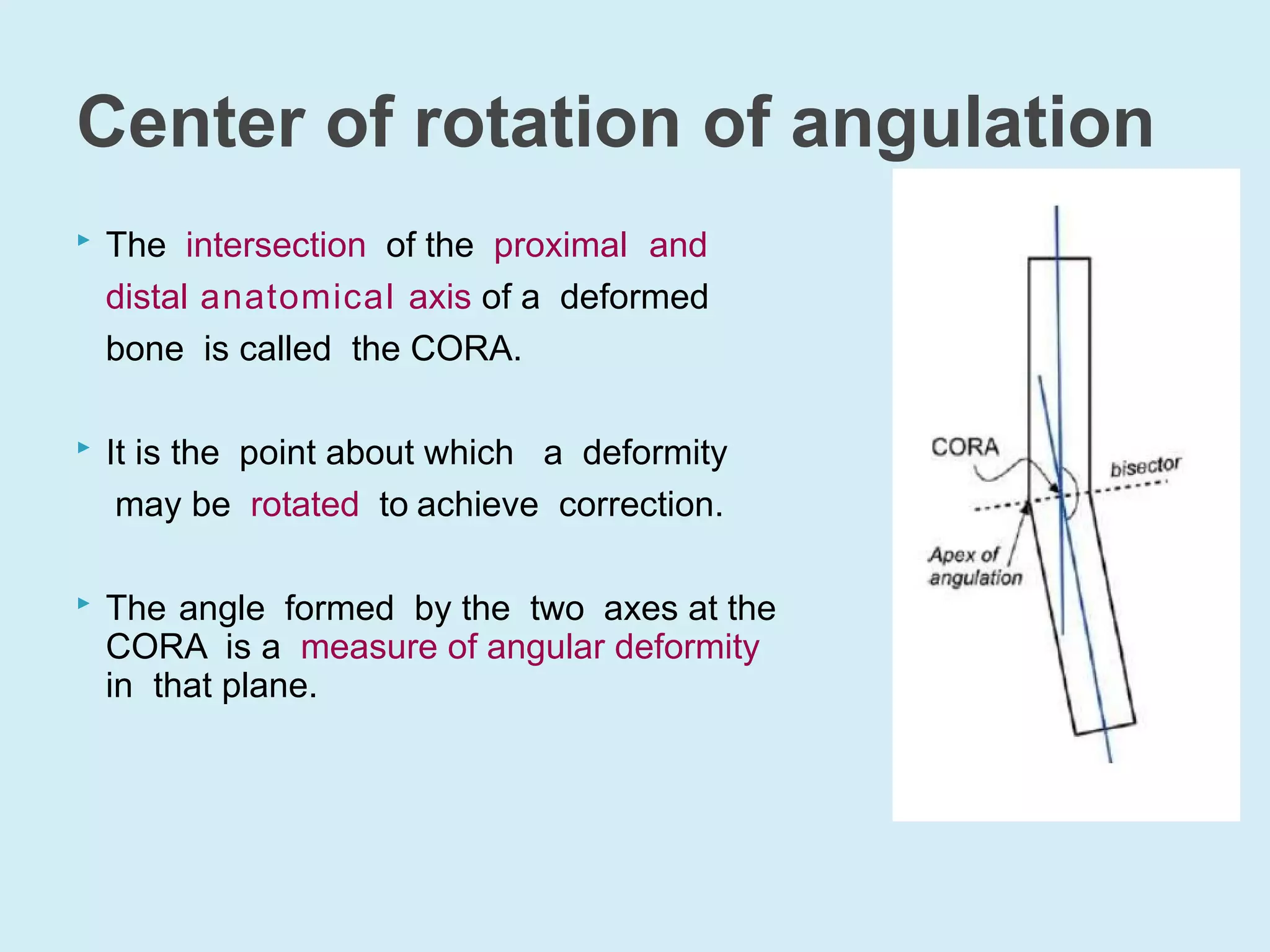
![ If CORA lies at the point of obvious deformity
in the bone and the joint orientations are
normal, the deformity is uniapical (in the
respective plane).[only angular deformity]
If CORA lies outside the point of obvious
deformity or either joint orientation is abnormal,
either a second CORA exists in that plane , the
deformityis multi-apical or translational deformity
exists in that plane.
When the CORA lies outside the boundaries of
the involved bone, a multi-apical deformity is
likely to be present.
Importance of CORA](https://image.slidesharecdn.com/osteotomyaroundkneedrshankarjangid1-190707063819/75/Osteotomy-around-knee-dr-shankar-jangid-1-15-2048.jpg)
![ A. The CORA, the correction axis, and the
osteotomy all lie at the same location; the
bone realigns through angulation alone,
without translation. [indicate only angular
deformity]
B. The CORA and thecorrection axis lie in the
same location but the osteotomy is proximal
or distal to that location; the bone realigns
through both angulation and translation.
C. The CORA lies at one location and the
correction axis and the osteotomy lie in a
different location; correction of angulation
results in an iatrogenic translational deformity.
Rule of osteotomy based on cora](https://image.slidesharecdn.com/osteotomyaroundkneedrshankarjangid1-190707063819/75/Osteotomy-around-knee-dr-shankar-jangid-1-16-2048.jpg)





![ Three different group..with different approach..
unicompartmental OA Knee..
patient with malalignment leg with ligament instability of knee..
patient with complex deformity...
Stage of osteoarthritis..
Patellofemoral joint involvement..
open wedge osteotomy[modified biplaner Tq]
Ligamentous instability..
persistant deformity+meniscectomy+along medial OA WITH varus..
posteriolateral instability+varus deformity...
Acl Pcl deficiency with intact lateral compartment...
Patient selection guidlines...](https://image.slidesharecdn.com/osteotomyaroundkneedrshankarjangid1-190707063819/75/Osteotomy-around-knee-dr-shankar-jangid-1-24-2048.jpg)

























![ Correction needed >20*
Flexion contracture>15*
Knee flexion <90*
Tibial subluxation >1cm
Medial compartment tibial bone loss>3mm
Patella baja
Inflammatory arthritis[RA]
Morbid obesity and smokers
Relative contraindication-age>60 yr..
Contraindication of high tibial
osteotomy](https://image.slidesharecdn.com/osteotomyaroundkneedrshankarjangid1-190707063819/75/Osteotomy-around-knee-dr-shankar-jangid-1-59-2048.jpg)






![ Correction of frontal plane valgus deformity with
lateral unicompartmental OA knee. [conta-RA]
Correction of load imbalance in ligamentous instability
due to medial collateral ligament insufficiency.
Correction of lateral patellofemoral maltracking due to
valgus leg alignment.
Genu recurvatum secondry to paralytic poliomylitis.
Genu valgum may be congenital,idiopathic, or
secondry to trauma, or might be due to rickets or
osteomalacia.
Indication of scfo](https://image.slidesharecdn.com/osteotomyaroundkneedrshankarjangid1-190707063819/75/Osteotomy-around-knee-dr-shankar-jangid-1-66-2048.jpg)









































































