Downloaded 2,818 times
![Maternal Physiology in Pregnancy: Cardiovascular System(Test dose)[25 mg] [100 ml] [5 min][Prescribed dose] [250 to 1000mg](Usually 500 ml NS) Total dose infusion: infuse over 2 to 6 hours.](https://image.slidesharecdn.com/maternalphysiologyinpregnancyalter-110729035822-phpapp01/85/Maternal-Physiology-in-Pregnancy-35-320.jpg)

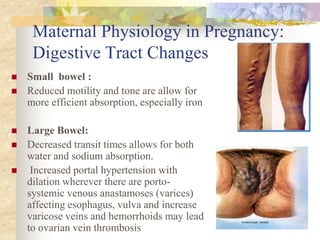
The document discusses major physiological adaptations in maternal anatomy, physiology, and metabolism during pregnancy, affecting nearly every organ system. It covers changes in nutritional needs, digestive tract function, urinary and cardiovascular systems, and various pregnancy-related symptoms. Understanding these physiological changes is essential for distinguishing normal pregnancy from pathological conditions.