
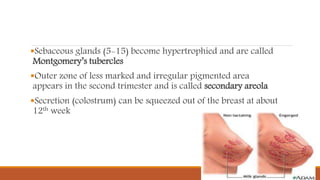
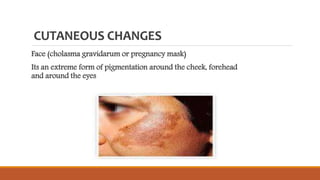


This document describes the physiological changes that occur in a woman's body during pregnancy. It discusses changes in the vulva, vagina, uterus, breasts, skin, blood, metabolism, respiratory and cardiovascular systems, urinary system, alimentary system, nervous system, and weight gain. The major changes include increased blood volume and cardiac output, softening of tissues like the cervix, hypertrophy of organs like the breasts, and temporary changes to skin pigmentation and the distribution of weight gain.

















































![Physiological and psychological changes during pregnancyhanges [Recovered].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/ppchangesrecovered-240119155912-065d14b8-thumbnail.jpg?width=640&height=640&fit=bounds)















































