Downloaded 493 times
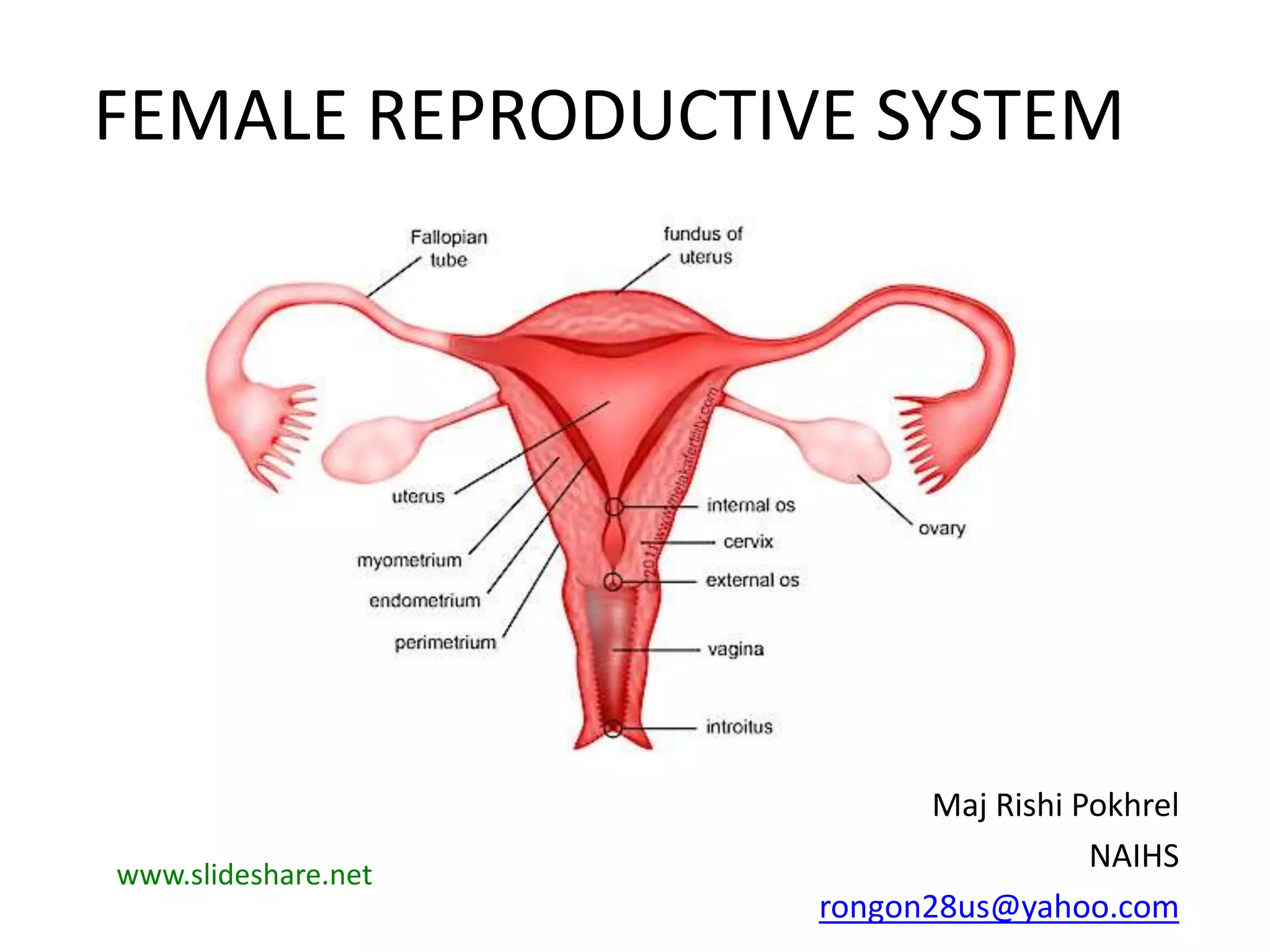
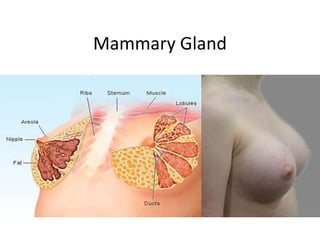

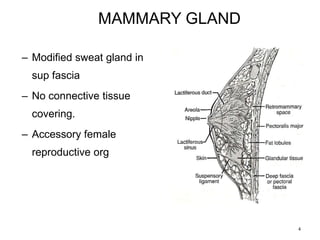
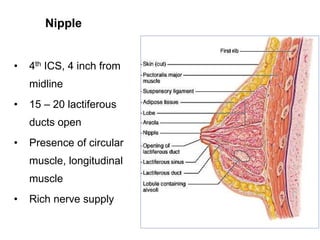
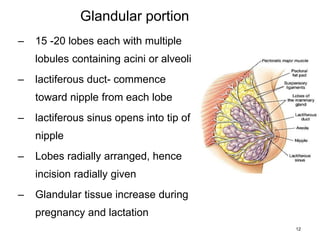
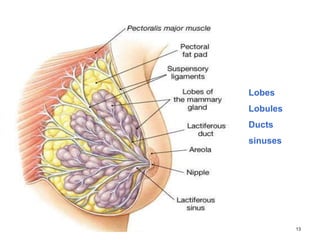
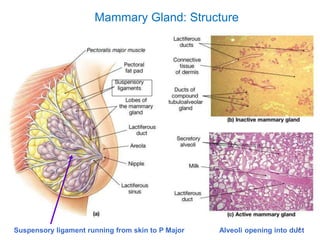
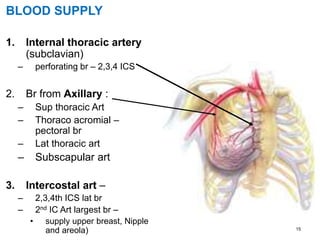
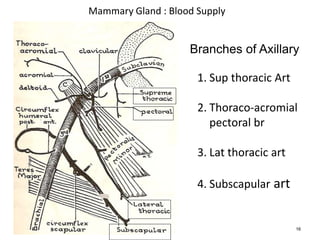
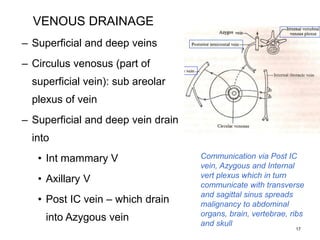
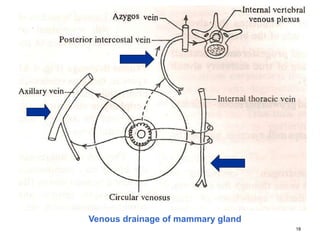
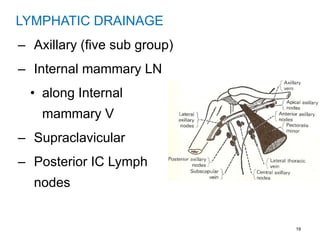



The female reproductive system document summarizes the anatomy of the mammary gland. It describes the location, shape, structure, blood supply, lymphatic and venous drainage of the mammary gland. The summary also discusses applied anatomy including common issues like breast cancer, infections, and congenital anomalies. Key points include that the mammary gland is made of 15-20 lobes containing lobules and alveoli, has blood supply from intercostal and thoracic arteries, and drains lymphatically to axillary lymph nodes.