Downloaded 197 times
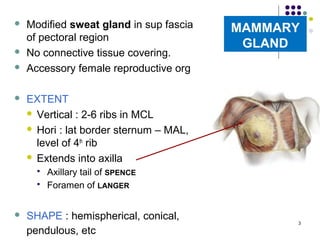
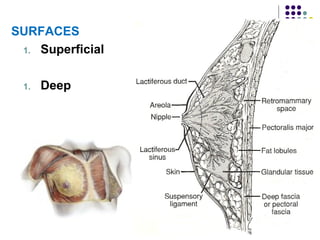
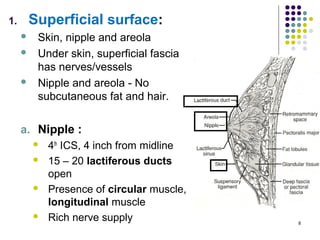
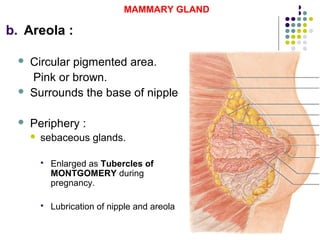
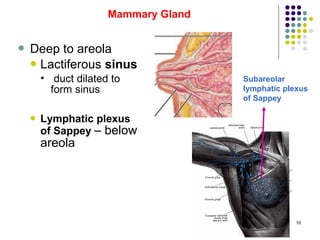
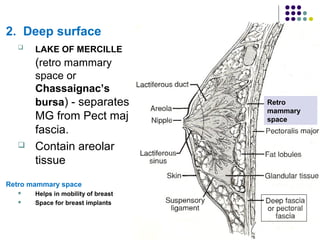
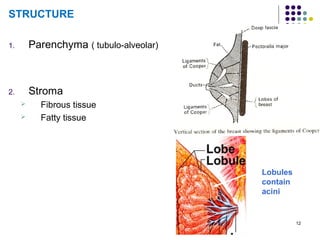
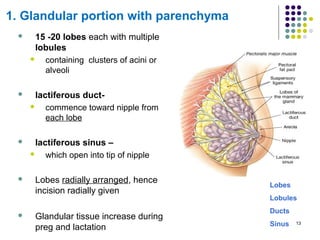
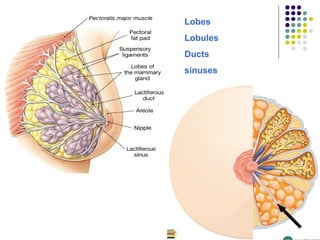
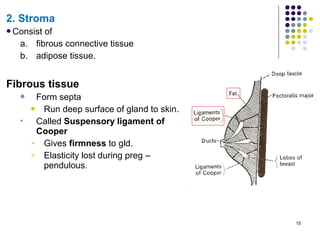
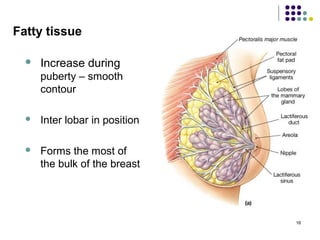
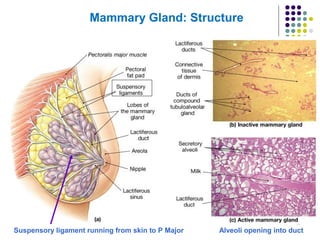
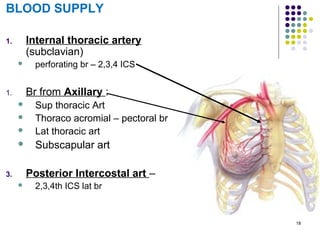
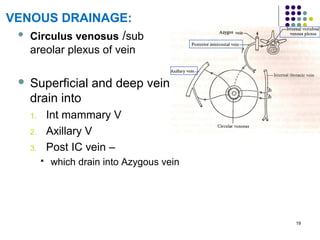
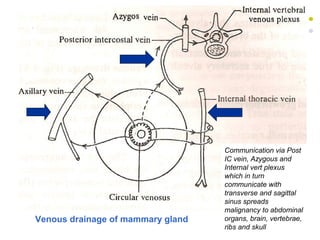
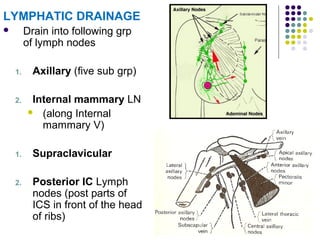
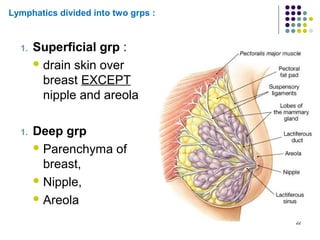
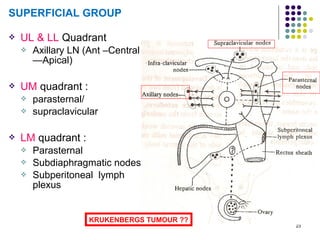
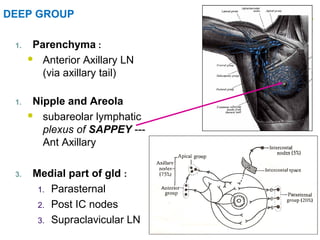
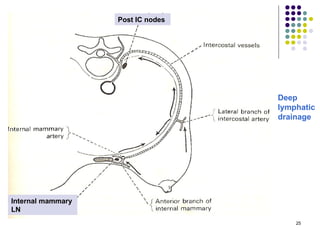
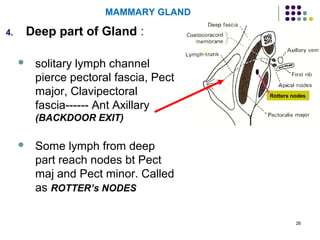
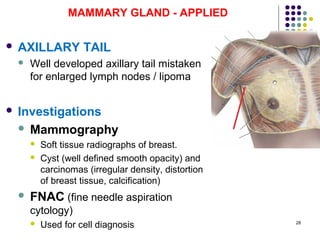
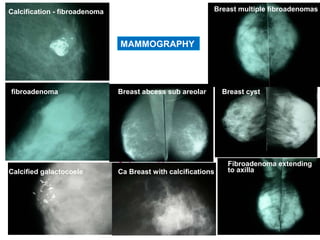


Maj Dr Poonam Singh's document provides an overview of the mammary gland. It discusses the gland's extent, surfaces, relations, structure, blood and lymphatic supply. The mammary gland is a modified sweat gland located in the sup fascia of the pectoral region. It has lobes containing lobules and lactiferous ducts that drain into sinuses opening at the nipple. The gland receives blood supply from intercostal and thoracoacromial arteries and drains lymphatically to axillary and internal mammary lymph nodes. Applied topics covered include infections, tumors, and management of breast cancer.













































































