Downloaded 297 times

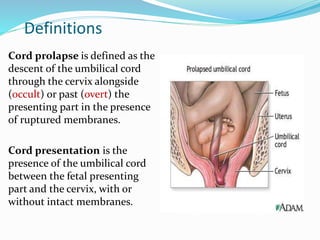














Cord prolapse occurs when the umbilical cord descends through the cervix ahead of the baby. It is a serious obstetric emergency that requires rapid diagnosis and management to prevent complications of cord compression cutting off blood supply to the baby. Immediate actions upon diagnosis include calling for assistance, preparing for an emergency c-section, and measures to relieve cord compression like elevating the baby. C-section is generally recommended for delivery unless vaginal birth is imminent. Community settings require rapid transfer to a hospital equipped for c-section. Delayed cord clamping can be considered if the baby is healthy after a complicated birth involving cord prolapse.



































































