Downloaded 181 times

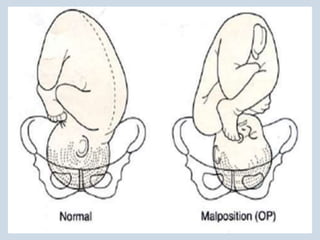
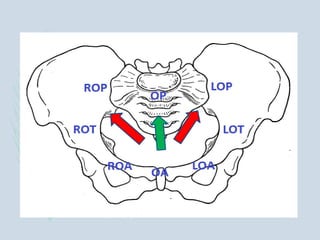
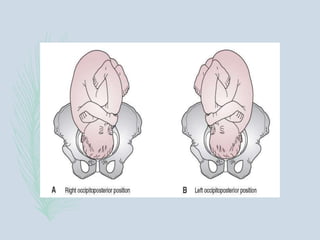
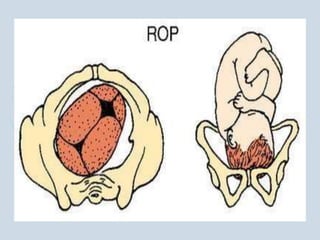
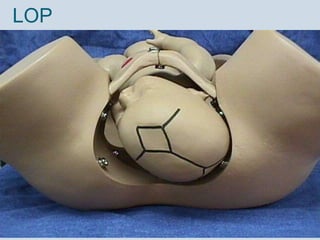

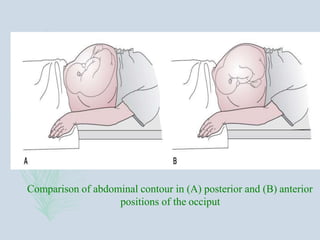
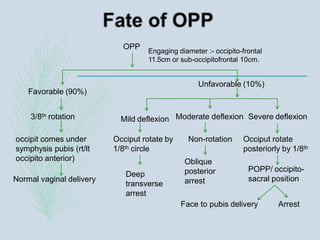
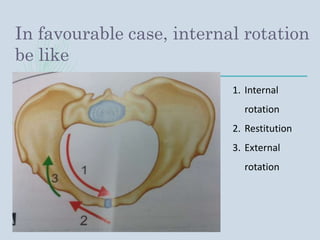
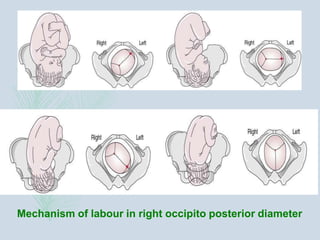
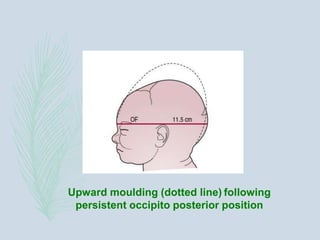
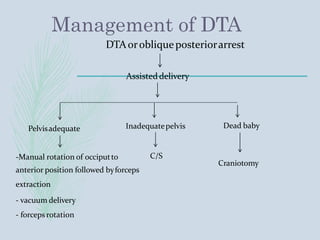
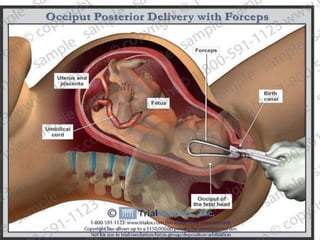



The document discusses occipito-posterior position, which refers to the vertex position where the occiput is placed posteriorly over the sacroiliac joint. Occipito-posterior occurs in approximately 10% of labors and can result from fetal or maternal factors that cause failure of internal rotation prior to birth. Successful vaginal delivery is possible if the occiput internally rotates anteriorly, but failure to rotate can cause complications requiring assisted delivery.









































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)













