MALPOSITION
“ Malposition refersto any
position of the vertex other than the
flexed occipito-anterior one.”
OCCIPITO POSTERIOR POSITION
“In a vertex presentation where
the occiput is placed posteriorly over
the sacroiliac joint, sacrum called
occipito-posterior postion.”
3.
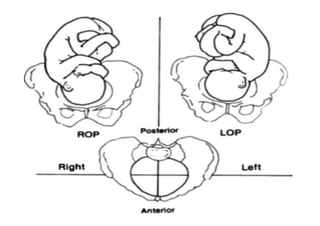
• Occiput placedover:- Right sacroiliac
joint called RIGHT OCCIPITO
POSTERIOR
• Occiput placed over:- Left sacroiliac
joint called LEFT OCCIPITO
POSTERIOR
• Traditionally called 3rd and 4rh position
of the vertex.
4.
• Occiput placedover:- sacrum called
DIRECT OCCIPITO POSTERIOR
• All the three positions are Primary
(before the onset of labour ) or
Secondary ( developing after labour
starts )
5.
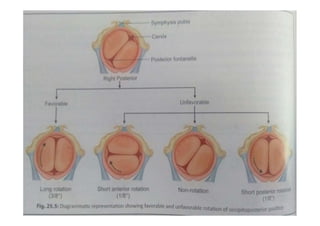
• In majorityof cases (90 %), ANTERIOR
ROTATION of occiput occurs and
follows the course like that of an
occipito anterior position and it is
favorable position
• But as the posterior position
occasionaly gives rise to dytocia, it is
described along with malpositions
7.
INCIDENCE
• At onsetof labour:- About 10 %
• Expected to be more during late
pregnancy and less during late second
stage of labour
• Right occipito posterior is 5 times more
common than the left occipito posterior
8.
• Dextro-rotation ofthe uterus and the
presence of sigmoid colon on the left,
disfavor Left Occipito Posterior
Position
• (Dextro-rotation is movement/rotation
to the right/ clockwise, opp. is
laevorotation)
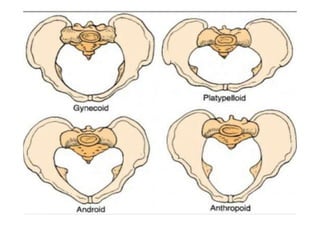
Shape ofthe pelvic inlet
More than 50 % cases are associated
with the ANTHROPOID OR ANDROID
PELVIC
The wide occiput can comfortably be
placed in the wider posterior segment
of the pelvis
12.
FETAL FACTORS
Markeddeflexion of the fetal head
Cuases of deflexion:-
1. High pelvic inclination (gedree
of slopping)
2. Anterior attachment of placenta
3. Primary bradycephaly
13.
• High pelvicinclination
–Inclination of brim is high and the
upper sacrum is relatively vertical
and convex
–Occiput will be placed to posterior
surface
14.
• Anterior attachmentof placenta
–Well flexed attitude but convexity of
maternal and fetal spine is opposite,
which leads to deflexion of fetal head
and thus the occiput with occupy the
posterior part
15.
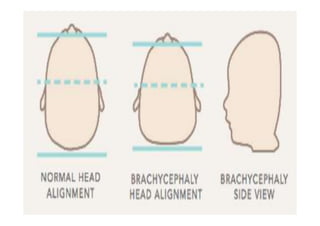
• Primary bradycephaly(flatened
area at back of the skull)
–Diminishes the effective movement
of flexion
17.
Uterine factor
Abnormaluterine contraction which
may be cause or effect, lead to
persistent deflexion and occipito
posterior postion
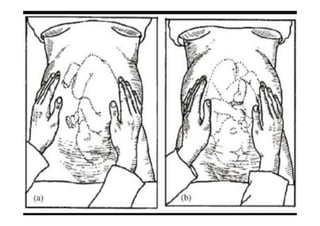
UMBILICAL GRIP
Fetallimbs are more easily palpable near
the midline on either side
The fetal back is felt far away from the
midline on the flank and often difficult to
outline clearly.
The anterior shoulder lies far away from
the midline
21.
PELVIC GRIP
Headis not engaged
Sinciput not felt as in well flexed occipito
posterior
AUSCULTATION
Intensity of fetal heart sound felt on the
flank and often difficult to locate
22.
VAGINAL EXAMINATION
Elongatedbag of membranes which is
likely to rupture during examination
Sagital suture occupies any obligue
diameters of the pelvis
Posterior fontanelle felt near the sacroiliac
joint
Anterior fontanelle felt more easily
because of deflexion of the head, lower
than posterior fontanelle
24.
MECHANISM OF LABOUR
•IN FAVOURABLE:
– Flexion
– Internal rotation of the head (head 3/8 ant.,
shoulder 2/8): occupy RIGHT oblidue
diameter in ROP and LEFT obligue
diameter in LOP
– Further descent : as occipito anterior p.
– Restitution
– External rotation
– Birth of the shoulders and trunk
25.
• IN UNFAVOURABLE:
–Incomplete forward rotation: deep
transverese arrest
– Non rotation
– Malrotation
27.
• Mechanism of“face to pubis” delivery
– Further descent occurs until the root of the
nose
– Flexion occurs
– Restitution
– External rotation
– Persistant occipito-posterior
28.
MANAGEMENT
• Early diagnosis
•Watchfull expectancy for decent and
anterior rotation
• Early cesarean section: Anticipating
prolonged labour, no progress of
labour, Persistant of deflexion and non-
rotation, Arrest labour, incoordinated
uterine contraction, fetal distress
29.
MANAGEMENT OF ARRESTOPP
1. Arrest in transverse / obligue occipito
posterior position:-
– Ventouse
– Alternative methods like mannual rotation
and extraction, cesarean section and
craniotomy
2. Occipitosacral arrest:-
– Forceps application followed by etraction
as face-to-pubis
– Liberal mediolateral episiotomy should be
done
30.
DEEP TRANSVERSE ARREST
•The head is deep in to the cavity,
sagital suture is placed in the
transverse bispinous diameter and
there is no progress in descent of the
head even after 0.5 to 1 hour following
full dilatation of the cervix
31.
CUASES
• Pelvic structure
•Deflexion of the head
• Weak uterine contraction
• Laxity of pelvic floor muscles
32.
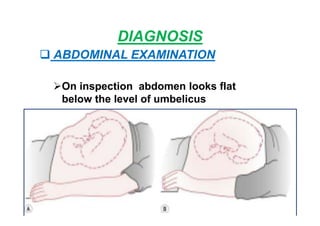
DIAGNOSIS
• Head isengaged
• Sagital suture lies in transverse
bispinous diameter
• Anterior fontanelle is palpable
• Faulty pelvic architecture
33.
MANAGEMENT
• If Vaginaldelivery not safe: Cesarean
section
• If Vaginal delivery safe: ventouse,
mannual rotation, forcep rotation
34.
MANNUAL ROTATION OFOPP
• The mannual rotation can be
accomplished with whole hand method
or with half hand method.
Steps:-
Put the patient under general anesthesia
Provide lithotomy position
Maintain full surgical asepsis
Catheterizaion should be done
Identify direction of occiput by PV Exa.
35.
• WHOLE HANDMETHOD:-
Step I: Gripping of the head
Step II: Rotation of the Head
Step III: Application of forceps
36.
Step I: Grippingof the head
In ROP or ROT the Left hand and in LOP or
LOT the Right hand is usually used.
The correctsponding hand is introduced
into the vagina in cone shapped manner
after seperating the labia by two fingers of
other hand.
37.
In Occipito transverseposition, the four
fingers are pushed in the sacral hollow to
be placed over the posterior parital bone
and the thumb is placed over the anterior
parital bone.
In oblique posterior position, four fingers
of patially supinated hand are placed over
the occiput and the thumb is placed over
the sinciput.
38.
Step II: Rotationof the head
Slight disimpaction may be needed for
good grip.
By the movement of pronation of the hand,
the head is rotated to bring the occiput
anterior along the shortest route.
Simultaneouslty, the back of the fetus is
rotated by the external hand from the flank
to the midline.
39.
This is anessential prerequisite, for
anterior rotation of head.
A little over rotation is desirable
anticipating slight recurrence of
malposition before the application of
forceps.
40.
In theAlternative
method, the four
fingers of the
pronated right hand
are placed over the
sinciput and the
thumb over the
occiput in ROP. The
head is rotated in the
supination movement
of the hand.
41.
Step III: Applicationof the forceps
Following Rotation, when the right hand is
placed over the left side of the pelvis, left
blade of the forcep is introduced.
When the left hand is used, it is placed on
the right side of the pelvis after rotation, as
such the right blade is to be introduced
first and the left blade is then to be
introduced underneath the right blade.
42.
While introducing theblades, it is
preferable that an assistant fixes the head
by suprapubic pressure in a manner of
first pelvic grip.
As it is a mid forceps application, axis
traction device should be used.
43.
DIFFICULTIES:-
Failure to gripthe head adequetly due to
lack of space
Failure to dislodge the head from the
impacted position
Inadequate anesthesia
Wrong case selection
44.
DANGERS-
Accidental slipping ofthe head above the
pelvic brim and prolapse of the cord
It is better to be perform cesarean section
in such a situation.
45.
• Half HANDMETHOD:-
Steps:
The rotation is done only by using the
right hand.
The four fingers are introduced into the
vagina and tangential pressure is applied
on the head at the level of diameter of
engagement.
46.
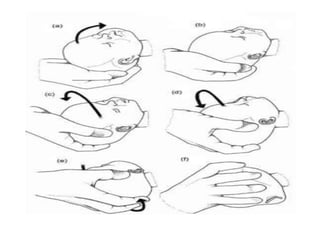
The pressure isapplied on the side and
the parietal eminence of the head.
In ROP or ROTpositions, the fingers are
placed anterior to the head and the
pressure is applied by the ulnar border of
the hand.
In LOP or LOT positions, the fingers are
placed posteriorly and the pressure is
applied by the radial border of the hand.
47.
The force isapplied intermittently till the
occiput is placed behind the symphysis
pubis.