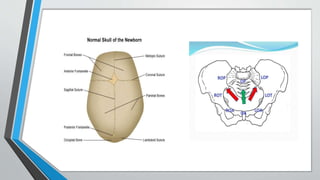
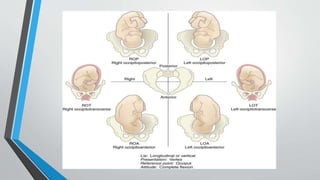
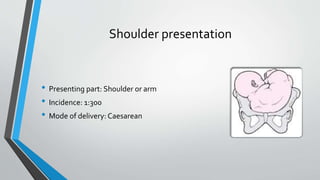
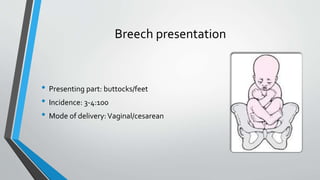
The document discusses malpresentation and malpositioning of the fetus during labor, particularly focusing on the occipito posterior position and its types, causes, and diagnosis. It outlines the mechanisms of labor in this malposition, the common management strategies for the first and second stages of labor, and various presentations of the fetus, including cephalic and breech presentations. Additionally, it addresses the complications associated with these positions and presents management options such as cesarean section, vacuum extraction, and manual rotation.