Downloaded 55 times































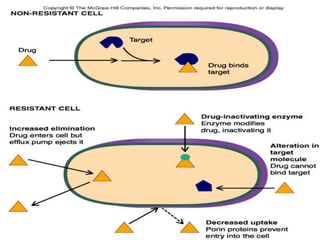





This document provides an introduction to principles of anti-microbial therapy. It discusses key topics including: - Sir Alexander Fleming's discovery of penicillin in 1928. - The definition of chemotherapy and agents used to treat infections and cancer. - Factors considered in selecting appropriate anti-microbial agents, including the infecting organism, site of infection, and patient factors. - Mechanisms of anti-microbial resistance that can develop, including genetic alterations in microbes and changes in target sites or drug accumulation. - Complications of anti-microbial therapy like hypersensitivity, direct toxicity, and superinfections.























































































