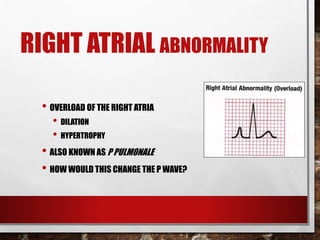
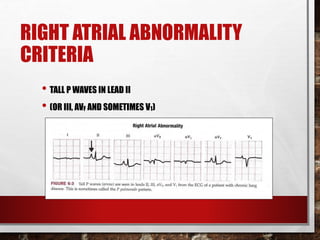
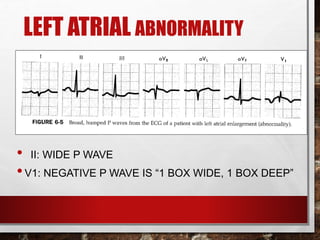
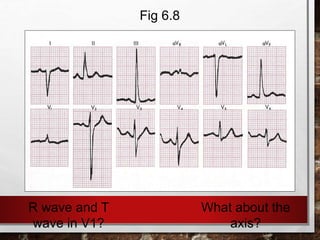
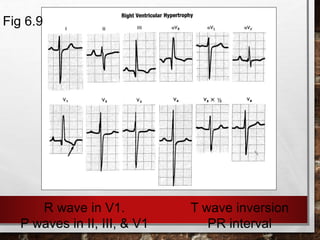
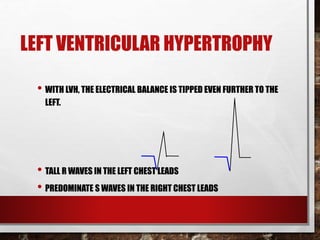
The document discusses atrial and ventricular enlargement, detailing the characteristics and criteria for identifying right and left atrial abnormalities and ventricular hypertrophy through ECG patterns. It outlines how changes in the P wave indicate right atrial hypertrophy and left atrial abnormality, as well as criteria for diagnosing right and left ventricular hypertrophy, including voltage measurements and associated conditions. Causes of these abnormalities are also covered, including pulmonary and valve diseases, hypertension, and congenital heart disease.