Download to read offline

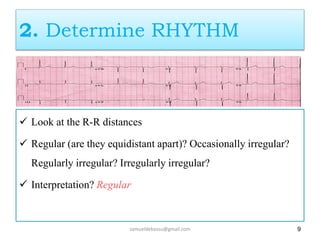
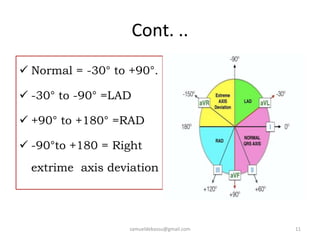
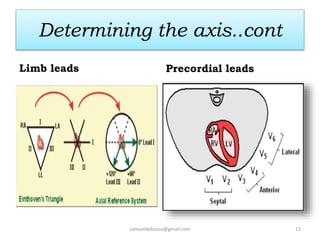
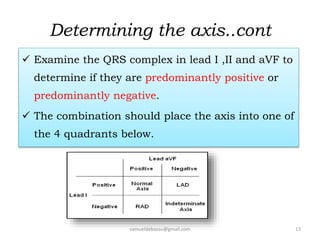
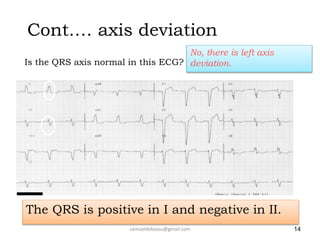
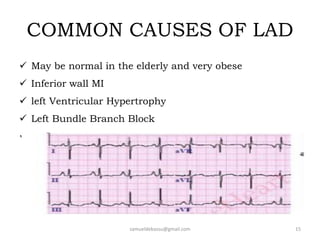

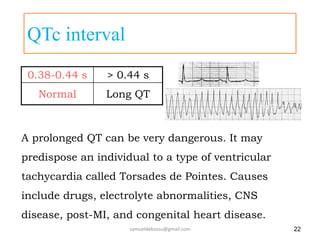
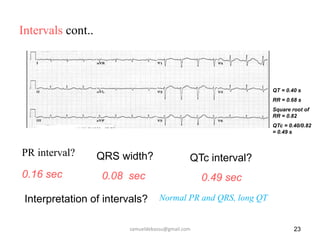
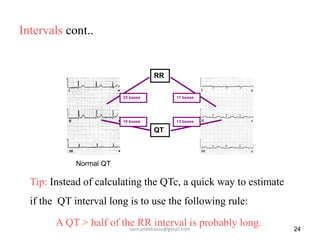
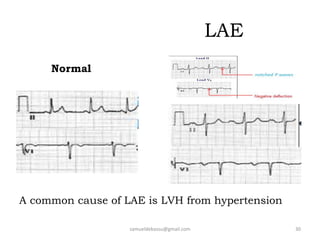
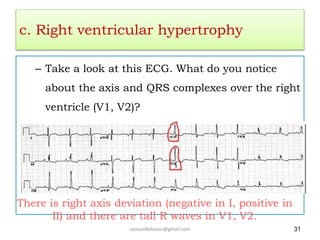
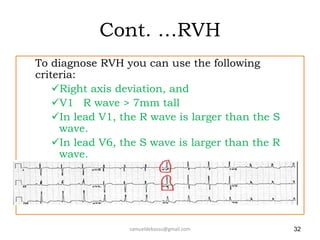
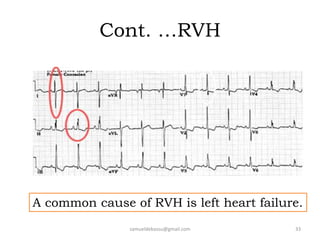
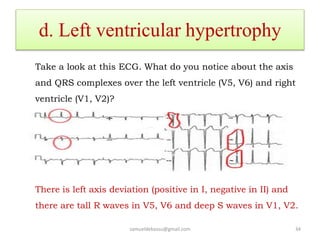
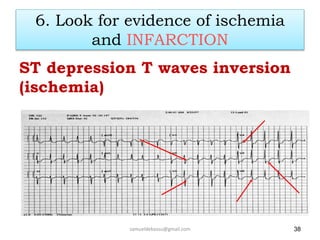
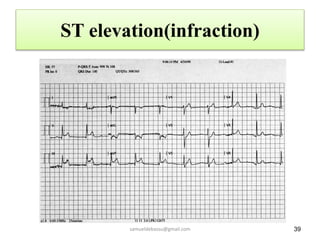
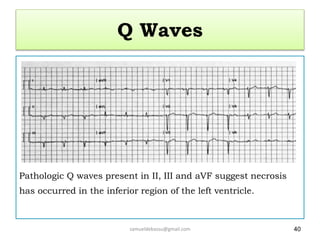
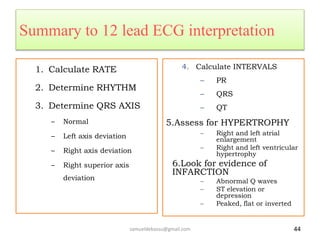


This document provides guidance on interpreting 12-lead electrocardiograms (ECGs). It discusses calculating the heart rate and determining the rhythm from the ECG. It outlines the steps to assess the electrical axis, measure intervals like PR and QT, evaluate for hypertrophy, and identify signs of ischemia or infarction. Common abnormalities are described, including left and right axis deviation, bundle branch blocks, and left ventricular hypertrophy. The summary emphasizes interpreting the ECG involves calculating the rate, assessing the rhythm, axis, intervals, hypertrophy, and looking for evidence of heart disease.



































































