Downloaded 95 times

![References
• Rahman A, Isenberg DA. Systemic lupus erythematosus. N Engl J Med. 2008;358(9):929-39.
• Bartels CM. Systemic Lupus Erythematosus (SLE). Medscape News [serial online]. November 15, 2011; Accessed December 16, 2011. Available at
http://emedicine.medscape.com/article/332244-overview
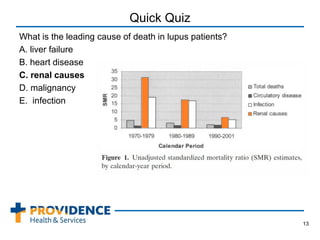
• Bernatsky S, Boivin JF, Joseph L, et. al. Mortality in systemic lupus erythematosus. Arthritis & Rheumatism 2006; 54: 2550–2557.
• Alarcón GS, McGwin G Jr, Bastian HM, Roseman J, Lisse J, Fessler BJ, et al. Systemic lupus erythematosus in three ethnic groups. VII [correction of
VIII]. Predictors of early mortality in the LUMINA cohort. LUMINA Study Group. Arthritis Rheum. 2001;45(2):191-202.
• Lupus Foundation of America. Lupus Fact Sheet. http://www.lupus.org/webmodules/webarticlesnet/templates/new_newsroomnews.aspx?articleid=351
&zoneid=59. Accessed December 16, 2011.
• Hochberg MC. Updating the American College of Rheumatology revised criteria for the classification of systemic lupus erythematosus. Arthritis
Rheum.1997;40(9):1725.
• Weening JJ, D'Agati VD, Schwartz MM, et al. The classification of glomerulonephritis in systemic lupus erythematosus revisited. J Am Soc Nephrol.
2004;15(2):241-50.
• Yazdany J, Panopalis P, Gillis JZ, Schmajuk G, MacLean CH, Wofsy D, et al. A quality indicator set for systemic lupus erythematosus. Arthritis Rheum.
2009;61(3):370-7.
• Navarra SV, Guzmán RM, Gallacher AE, Hall S, Levy RA, Jimenez RE, et al. Efficacy and safety of belimumab in patients with active systemic lupus
erythematosus: a randomised, placebo-controlled, phase 3 trial. Lancet. 2011;377(9767):721-31.
• Hill E. Belimumab Earns FDA Approval for Lupus. Medscape News [serial online]. March 15, 2011;Accessed December 16, 2011. Available at
http://www.medscape.com/viewarticle/738729.
• Appel GB, Contreras G, Dooley MA, et al. Mycophenolate mofetil versus cyclophosphamide for induction treatment of lupus nephritis. J Am Soc
Nephrol. 2009;20(5):1103-12.
• Isenberg D, Appel GB, Contreras G, et al. Influence of race/ethnicity on response to lupus nephritis treatment: the ALMS study. Rheumatology (Oxford).
2010;49(1):128-40.
• Delafuente JC, Cappuzzo KA. Systemic Lupus Erythematosus and Other Collagen-Vascular Diseases. In: Dipro JT, Talbert RL, Yee GC, Matzke GR,
Wells BG, Posey LM, eds. Pharmacotherapy: A Pathophysiologic Approach. 7th ed. New York: McGraw-Hill Companies, Inc., 2008: 1431-1445.
• Lau AH. Glomerulonephritis. In: Dipro JT, Talbert RL, Yee GC, Matzke GR, Wells BG, Posey LM, eds. Pharmacotherapy: A Pathophysiologic Approach.
7th ed. New York: McGraw-Hill Companies, Inc., 2008: 811-831
• (Chapter). Joseph T. DiPiro, Robert L. Talbert, Gary C. Yee, Gary R. Matzke, Barbara G. Wells, L. Michael Posey: Pharmacotherapy: A
Pathophysiologic Approach, 7e: http://www.accesspharmacy.com/content.aspx?aID=3187202.
• Walsh N. Predictors of renal failure in systemic lupus erythematosus. MedPageToday [serial online]. November 14, 2011; Accessed December 16,
2011. Available at http://www.medpagetoday.com/MeetingCoverage/ACR/29660.
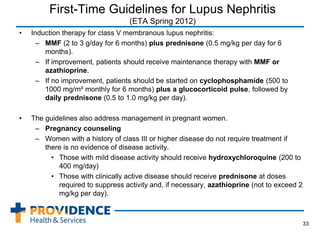
• Gordan D. First-Time Guidelines for Lupus Nephritis. Medscape News [serial online]. November 8, 2011; Accessed December 16, 2011. Available at
http://www.medscape.com/viewarticle/753134.
36](https://image.slidesharecdn.com/f59ed68b-9cb9-4bf0-989b-238d68666660-150504164623-conversion-gate02/85/lupus-presentation-final-36-320.jpg)

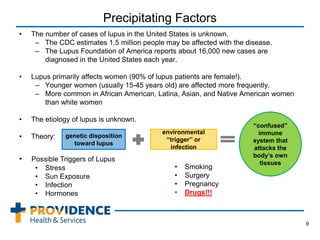
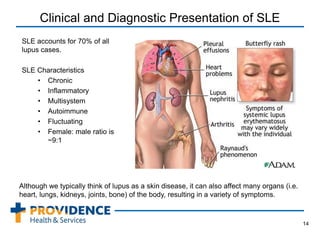
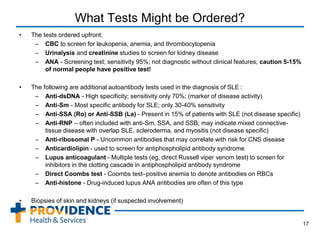
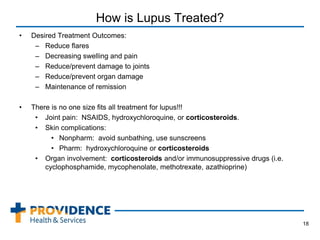
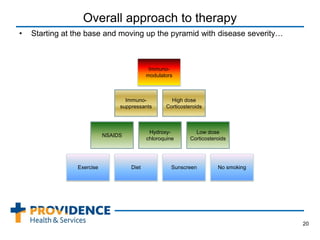
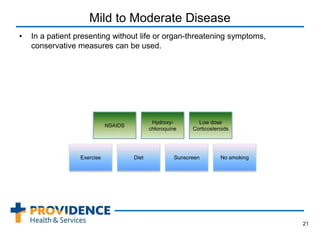
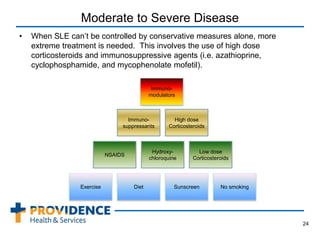
This document provides an overview of lupus, a chronic autoimmune disease that can affect multiple organs and tissues. It discusses the epidemiology of lupus, noting it primarily affects women and is more common in certain ethnic groups. The pathogenesis involves a genetic predisposition interacting with environmental triggers that result in an abnormal immune response attacking the body's own tissues. Symptoms and organ involvement can vary widely between patients. Diagnosis is based on meeting several criteria that may include rashes, arthritis, kidney disease, neurological issues, and positive antibody tests. Treatment depends on disease severity and organ involvement, ranging from lifestyle changes to immunosuppressive drugs and corticosteroids. Lupus nephritis, or kidney involvement,























































































