Downloaded 512 times







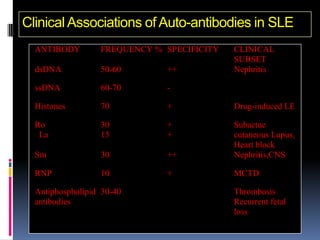
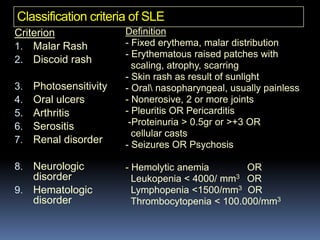
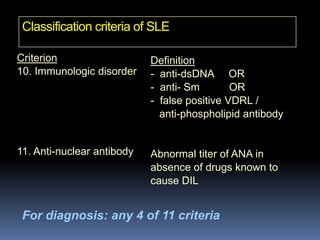


Systemic Lupus Erythematosus (SLE) is an inflammatory autoimmune disease characterized by excessive autoantibody production leading to tissue damage. It has a wide variety of clinical manifestations that can affect many different organ systems. Some key points: - SLE predominantly affects women of childbearing age and has a strong genetic component. Certain genetic and environmental factors can increase risk. - Clinical features include skin rashes, arthritis, kidney involvement ranging from mild proteinuria to severe nephritis, neurological/psychiatric symptoms, hematological abnormalities and involvement of other organs. - Diagnosis is based on identifying a combination of clinical and laboratory criteria including high titers of antinu



































































































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)







