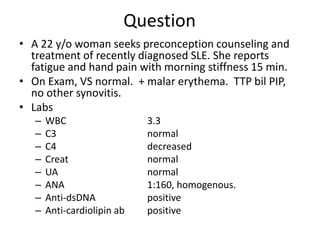
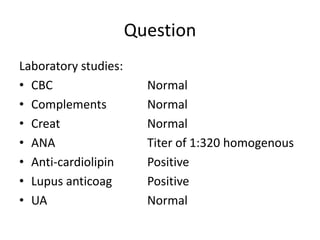
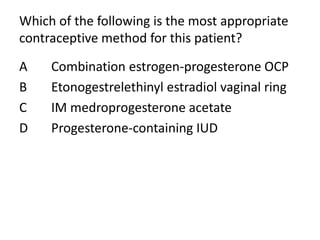
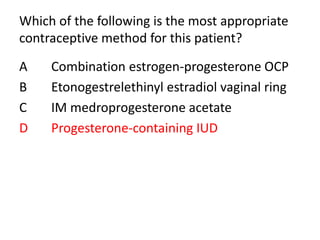
This patient has longstanding SLE with quiescent disease activity currently. She has a history of fetal loss and blood clots while pregnant previously. She is seeking contraceptive options other than barrier methods. Given her history of APL antibodies and blood clots, progesterone-only contraceptives like the progesterone IUD or depot medroxyprogesterone would be safest options to avoid estrogen which could increase her risk for further clotting issues.


























































![2019 04-30 noon conference [stephen slade]](https://cdn.slidesharecdn.com/ss_thumbnails/2019-04-30noonconferencestephenslade-190501212611-thumbnail.jpg?width=640&height=640&fit=bounds)



























![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)

