Download as PDF, PPTX


![Preferred HIV PEP Regimen
PEP is now recommended for ALL occupational exposures to HIV!
Raltegravir (Isentress: RAL) 400 mg PO twice daily
Plus
Truvada, 1 PO daily
(Tenofovir [Viread; TDF] 300 mg + emtricitabine [Emtriva; FTC] 200 mg)
Watch for Stribald (alternative therapy):
Stribild (elvitegravir, cobicistat, tenofovir DF, emtricitabine)
1 pill, once daily dosing
9](https://image.slidesharecdn.com/416763f5-77ce-4567-b422-ccab3bf134dc-150504165418-conversion-gate02/85/PEP-pearl-110413-9-320.jpg)
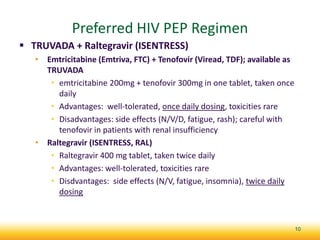



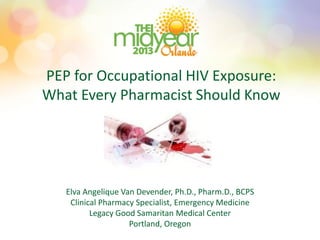

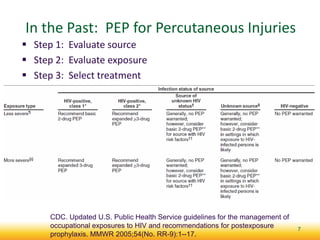
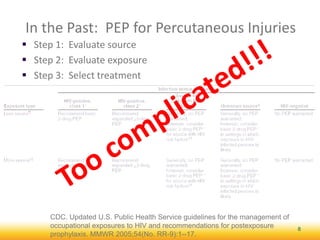
Truvada and raltegravir are the preferred regimen for occupational post-exposure prophylaxis (PEP) for HIV exposure. PEP should be started immediately after exposure and continued for 28 days to reduce the risk of HIV infection. Important follow up includes monitoring for side effects, adherence support, and HIV testing at baseline and over several months to evaluate infection status. Pharmacists play a key role in ensuring appropriate PEP regimens can be obtained and supporting patient adherence for full treatment duration.



























































