Downloaded 77 times
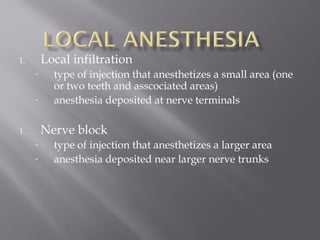
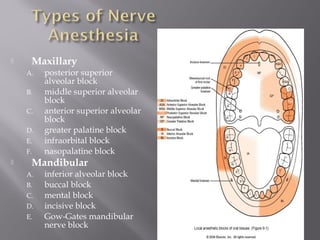
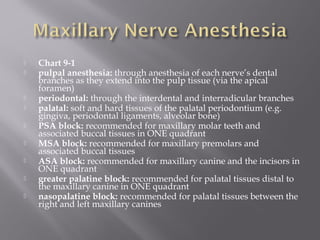
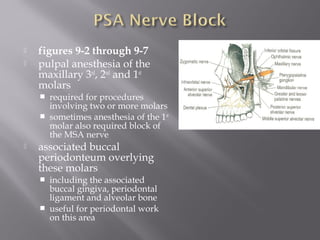
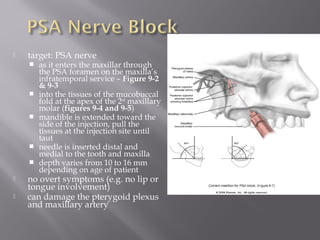
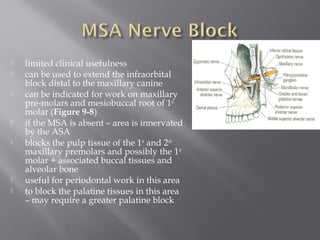
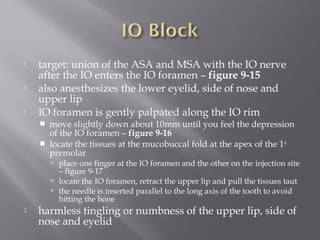
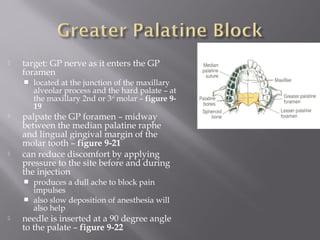
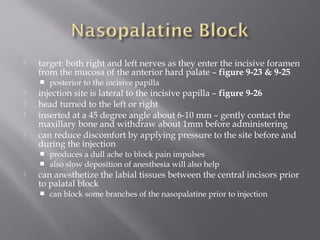
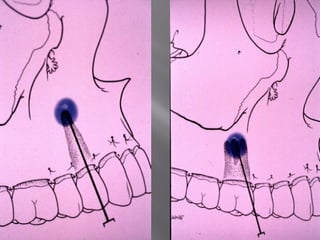
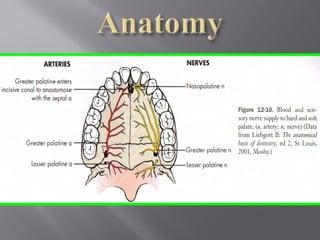
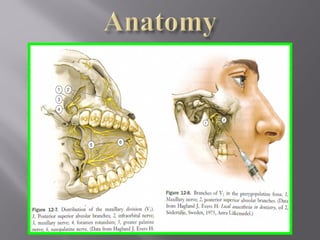

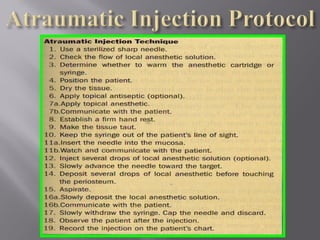
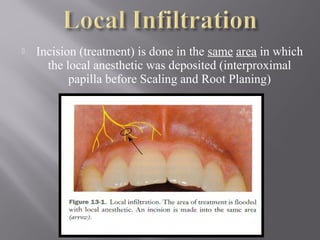
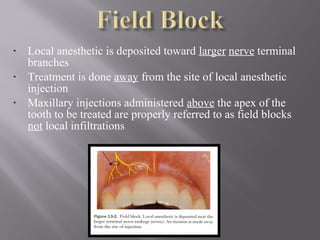
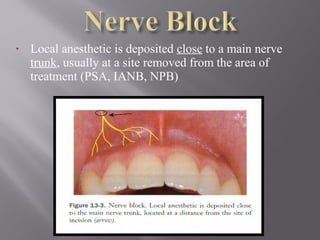
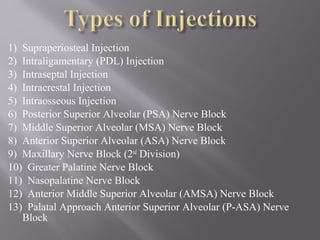
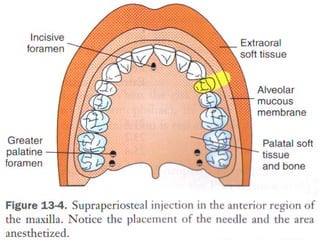
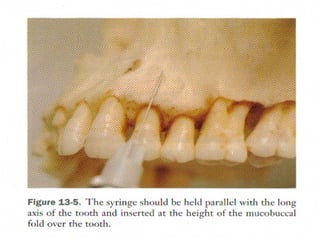
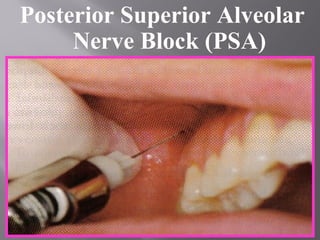
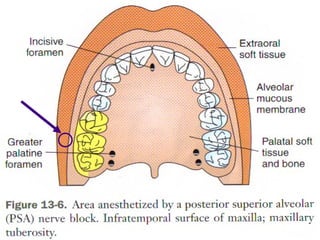
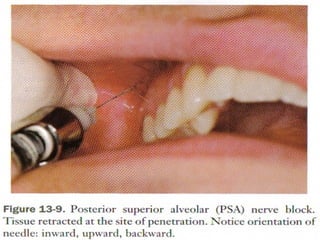
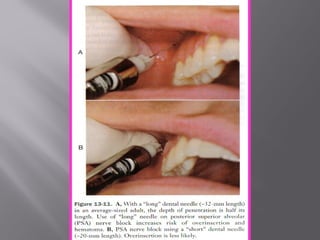
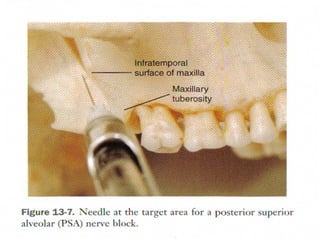
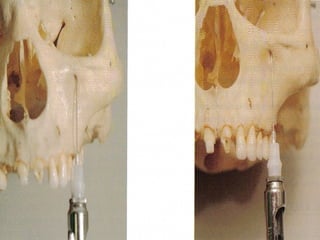
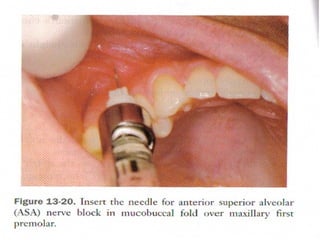
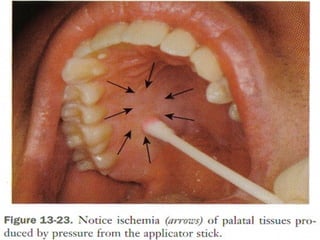
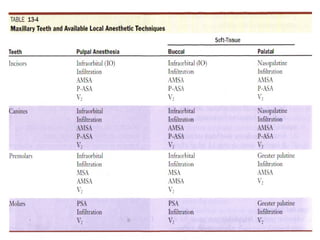
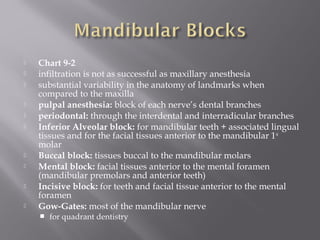
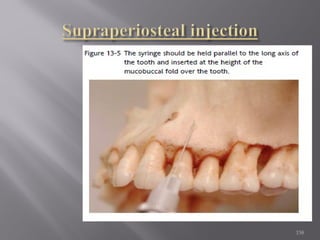
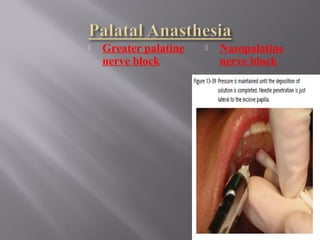





The document discusses various types of dental injections including local infiltration, nerve blocks, and field blocks. It provides details on specific injections for the maxilla, such as the posterior superior alveolar nerve block, which is used to anesthetize the maxillary first, second, and third molars. The document describes injection techniques, target areas, and expected outcomes for different maxillary injections.
































![Techniques of local anesthesia [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/techniquesoflocalanesthesiaautosaved-210618141111-thumbnail.jpg?width=640&height=640&fit=bounds)



































![Hypothalamus short notes on location, function and disorders by Dr. Neha [PT]...](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124142231-2b48143d-thumbnail.jpg?width=640&height=640&fit=bounds)


















