Downloaded 22 times
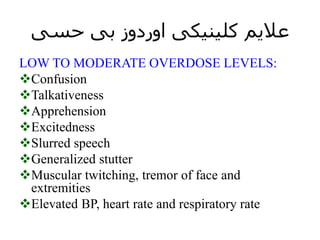
![Edema
If edema occurs in any area where it compromises breathing, treatment consists of the
following:
• P (position): if unconscious, the patient is placed supine.
• A-B-C (airway, breathing, circulation): basic life support is administered, as
needed.
• D (definitive treatment): emergency medical services (e.g., 9-1-1) is summoned.
• Epinephrine is administered: 0.3 mg (0.3 mL of a 1:1000 epinephrine solution)
(adult), 0.15 mg (0.15 mL of a 1:1000 epinephrine solution) (child [15 to 30 kg]),
intramuscularly (IM) or 3 mL of a 1:10,000 epinephrine solution intravenously (IV-
adult), every 5 minutes until respiratory distress resolves.
• Histamine blocker is administered IM or IV.
• Corticosteroid is administered IM or IV.
• Preparation is made for cricothyrotomy if total airway obstruction appears to be
developing. This is
• extremely rare but is the reason for summoning emergency medical services early.
• The patient's condition is thoroughly evaluated before his or her next appointment
to determine the cause of the reaction.](https://image.slidesharecdn.com/la7copmlicatin-170720114049/85/local-anesthesia-in-dentistry-7-copmlicatin-13-320.jpg)
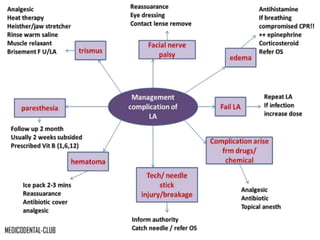
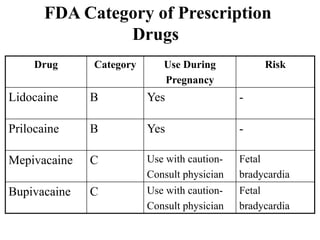


This document discusses local complications and systemic effects that can occur from the use of local anesthetics in dentistry. It describes various local complications including needle breakage, prolonged anesthesia, facial nerve palsy, trismus, soft tissue injury, hematoma, pain on injection, and infection. It then discusses signs and symptoms of local anesthetic overdose as well as factors that can contribute to overdose. Lastly, it provides guidance on controlling complications for special patient populations such as uncooperative children, pregnant women, and those receiving anticoagulation therapy.


















































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)



![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)
