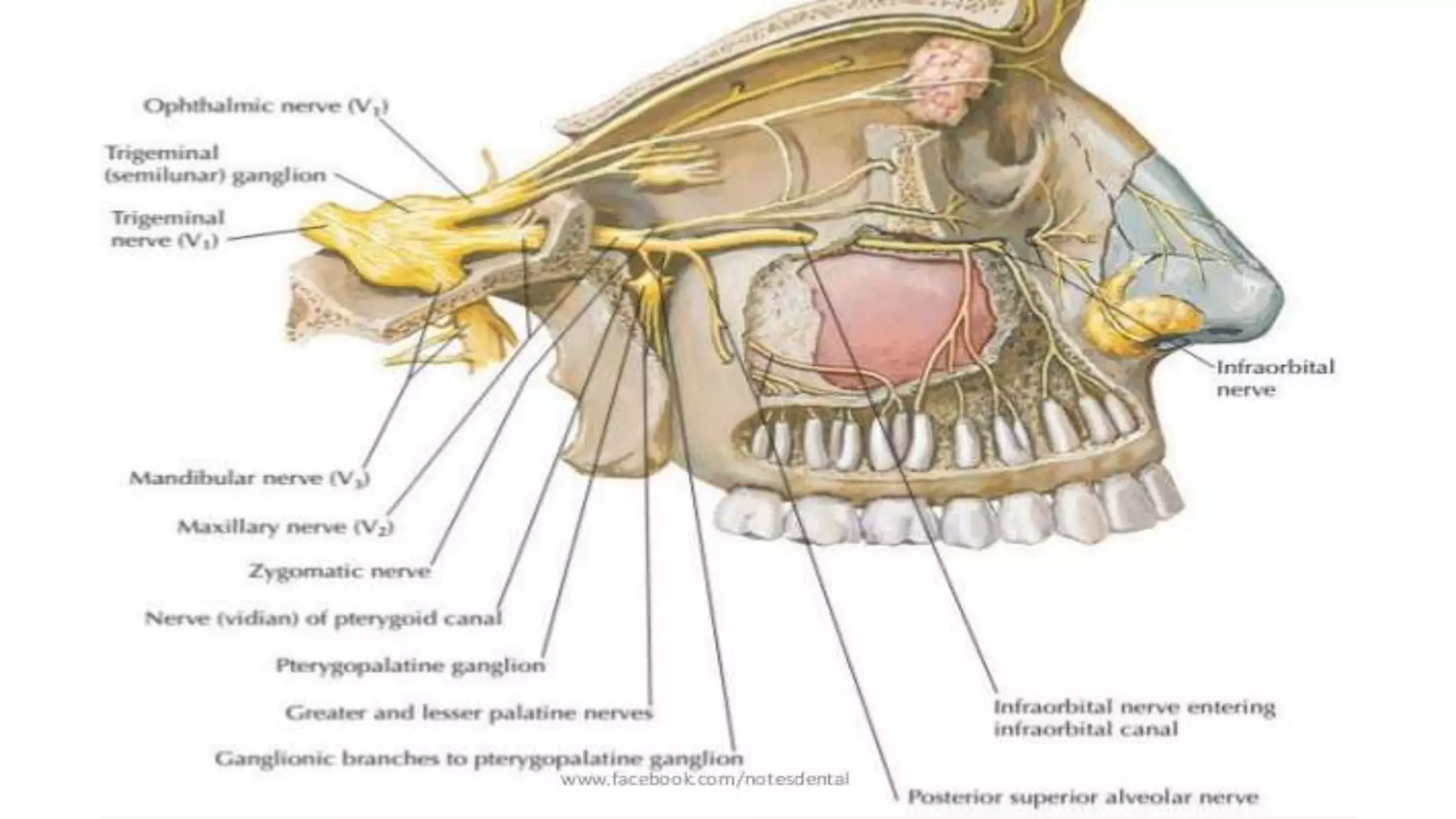
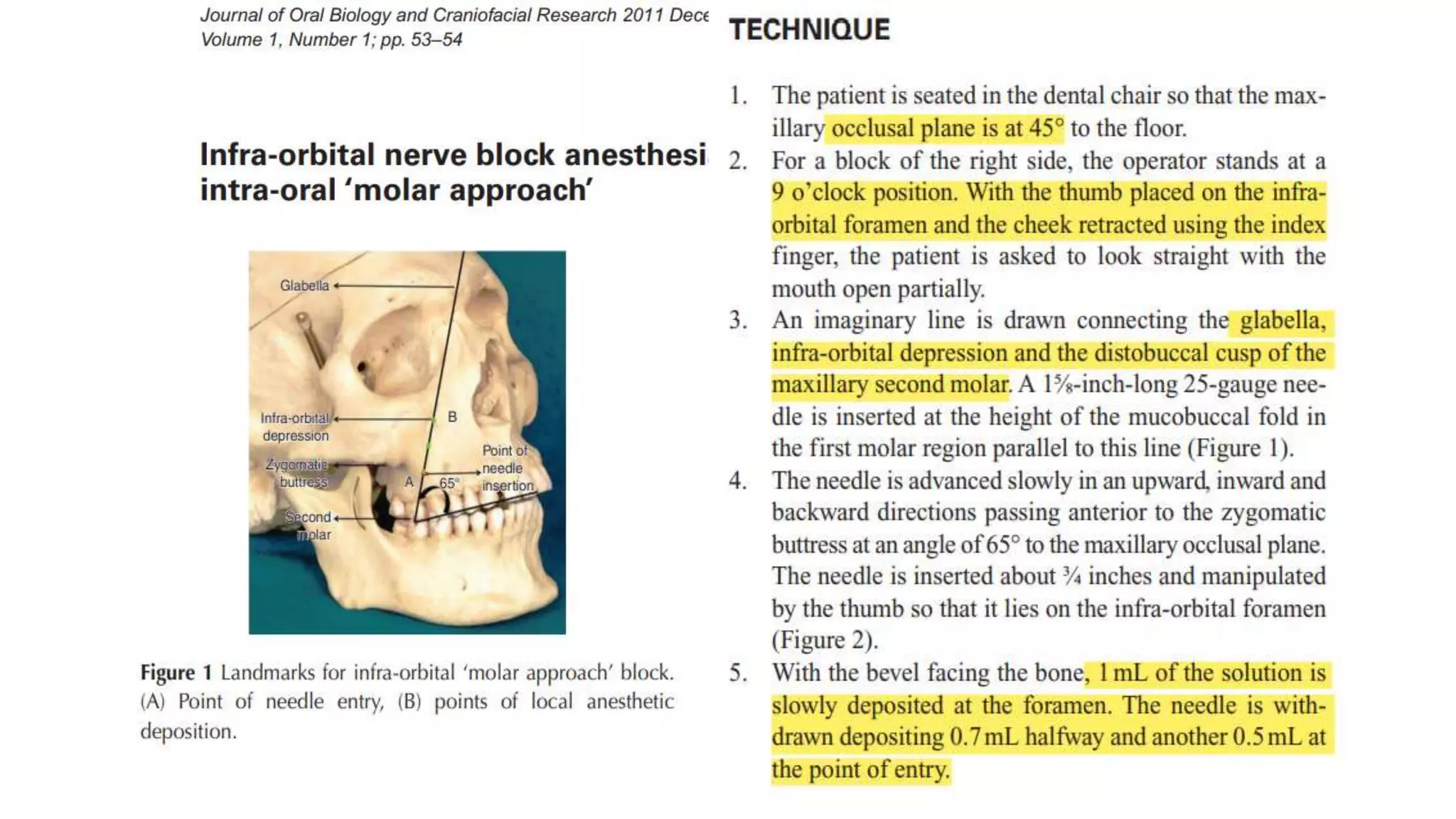
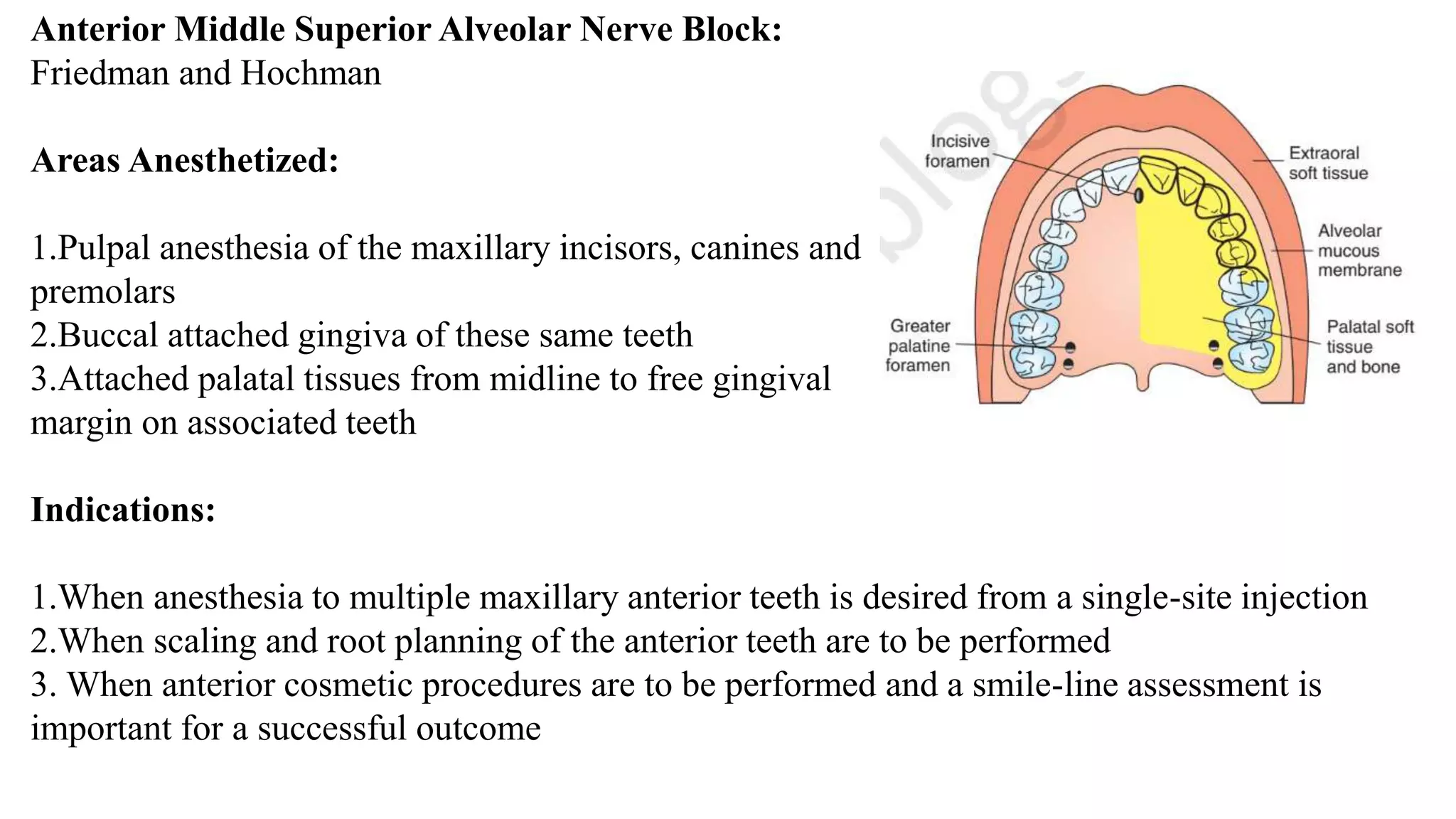
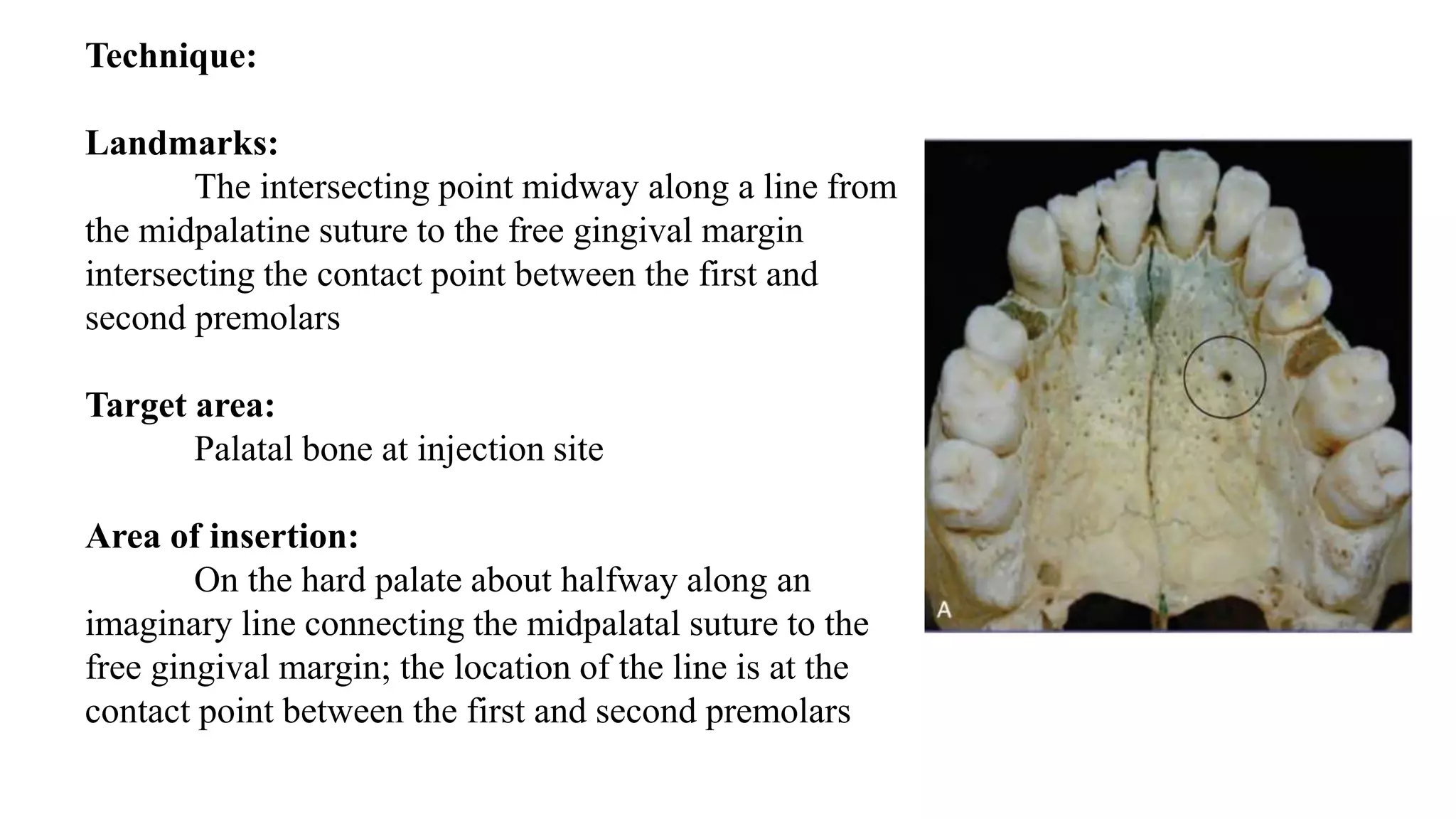
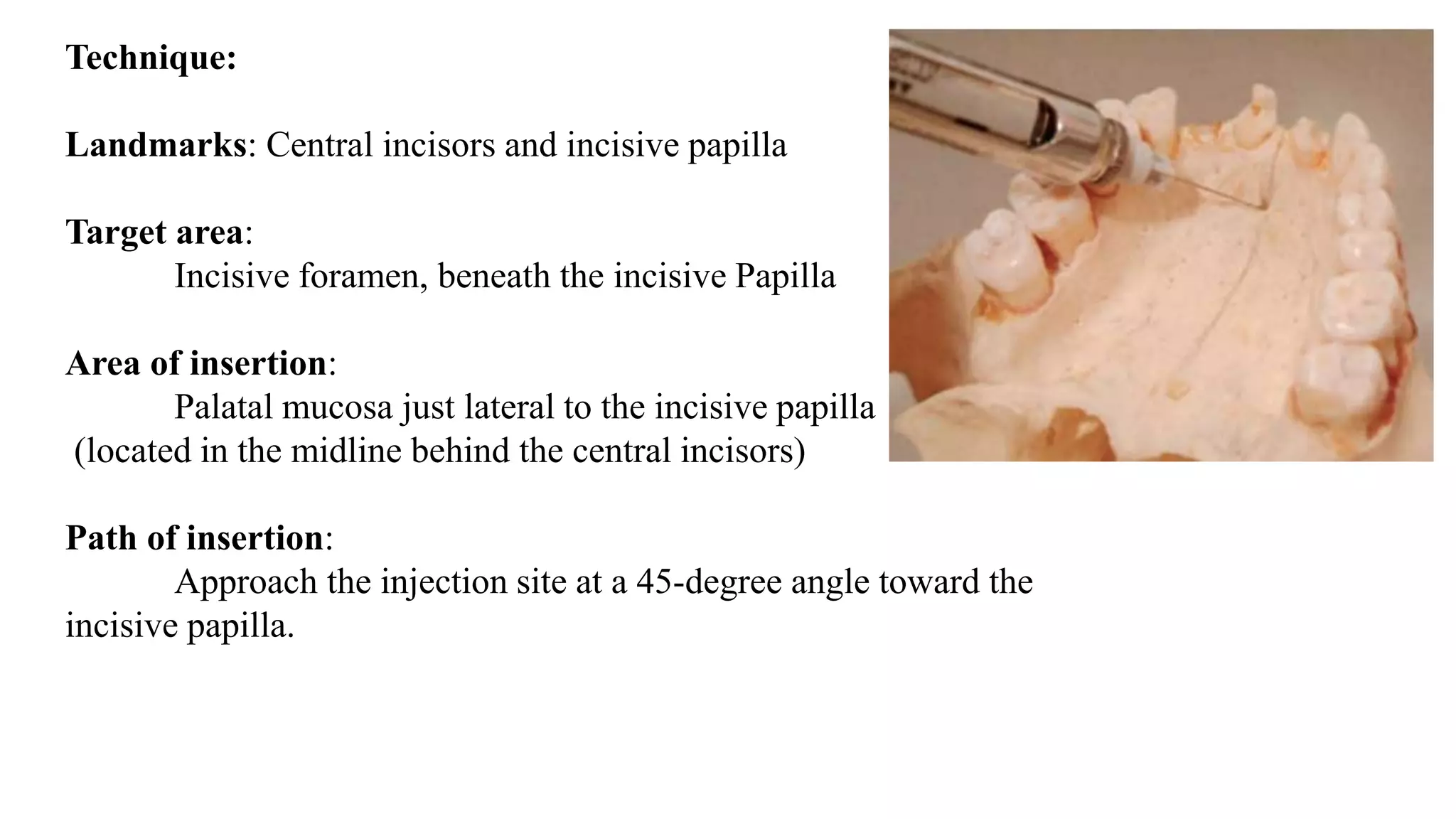
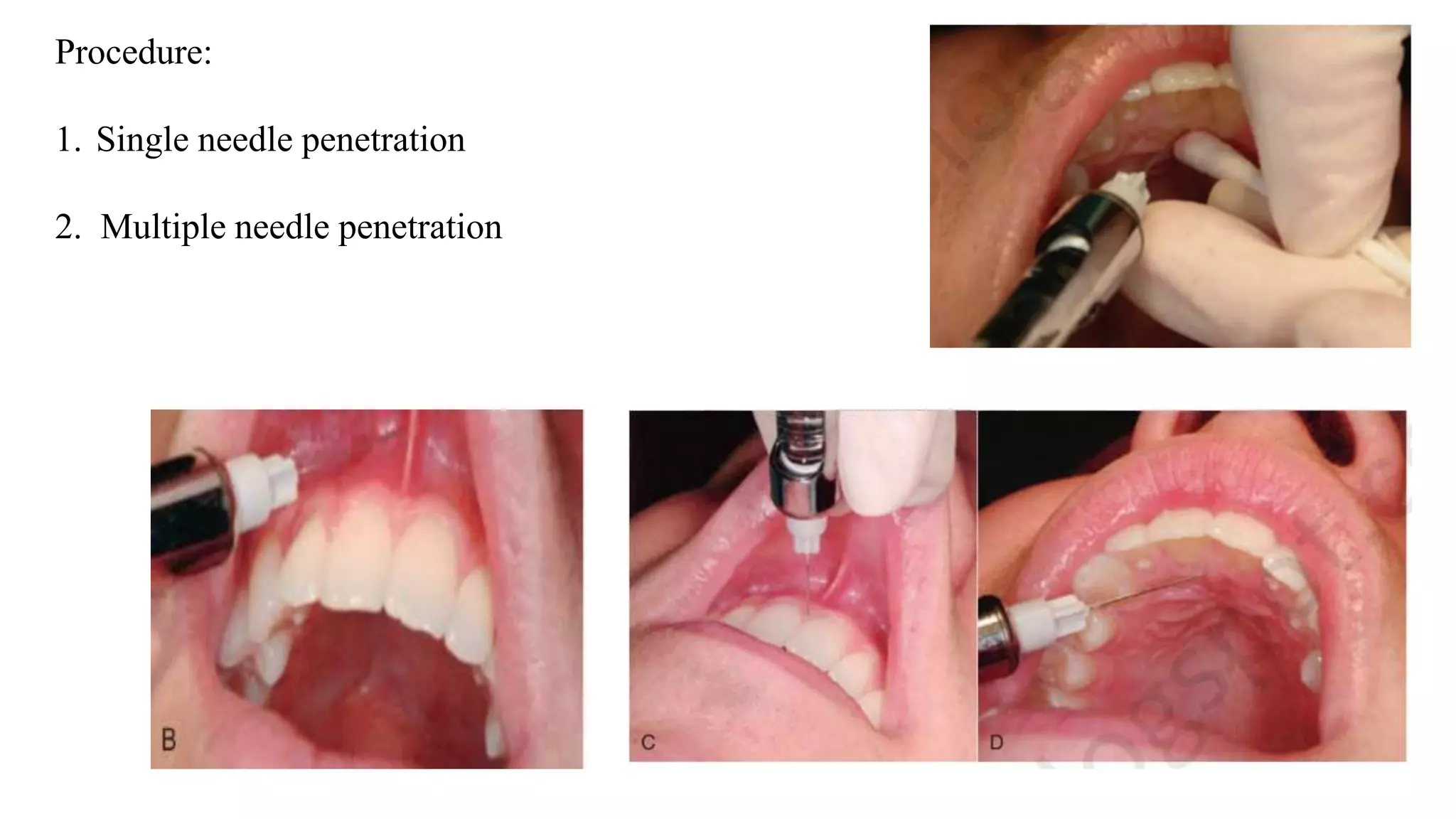
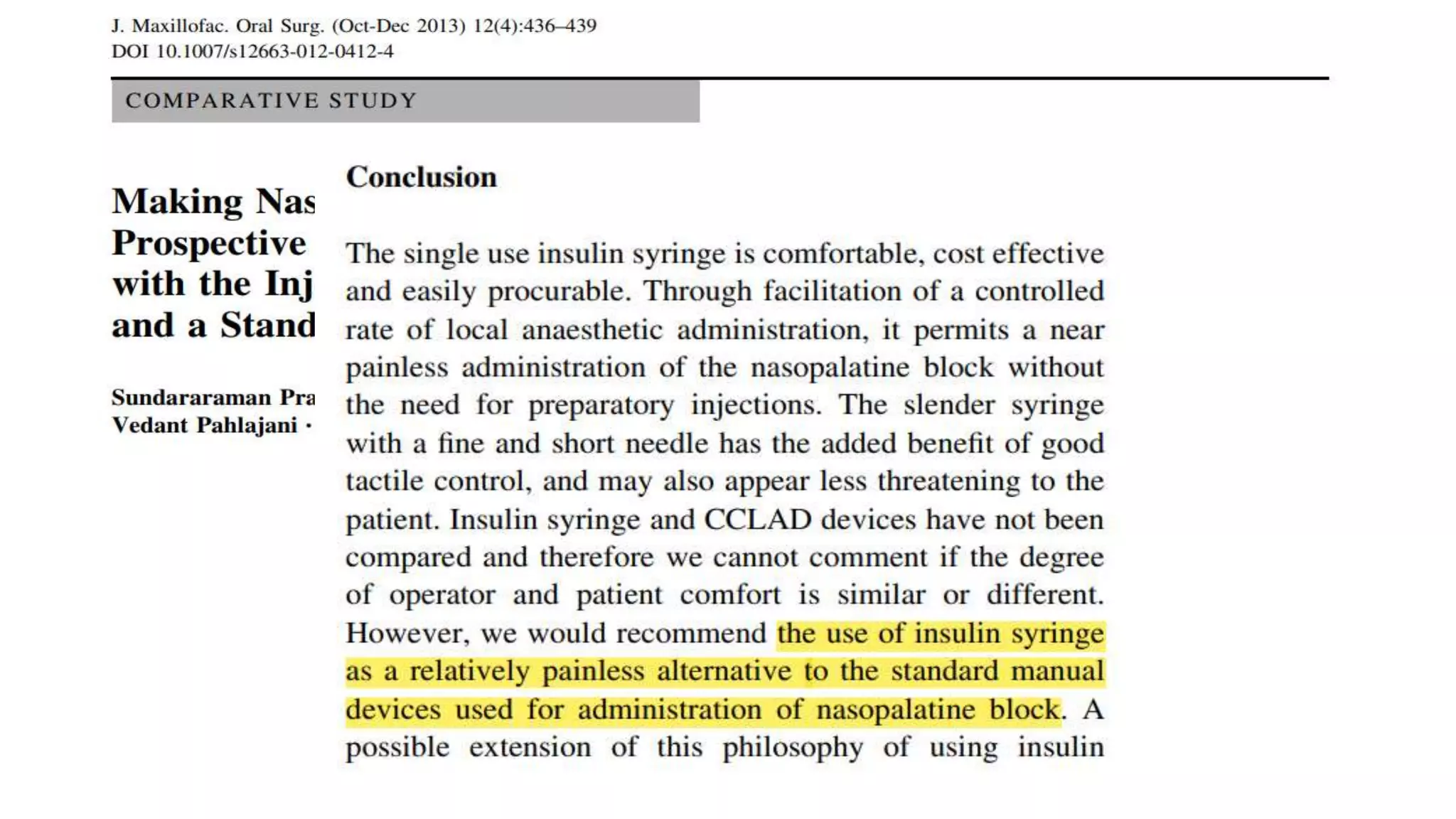
This document provides a comprehensive overview of maxillary nerve blocks, including anatomical details, local anesthesia techniques, and specific nerve block procedures. It outlines indications, techniques, complications, and management for various intra-oral and extra-oral techniques used in dental anesthesia. The document serves as a guide for dentists on effective pain management during dental procedures involving the maxillary region.
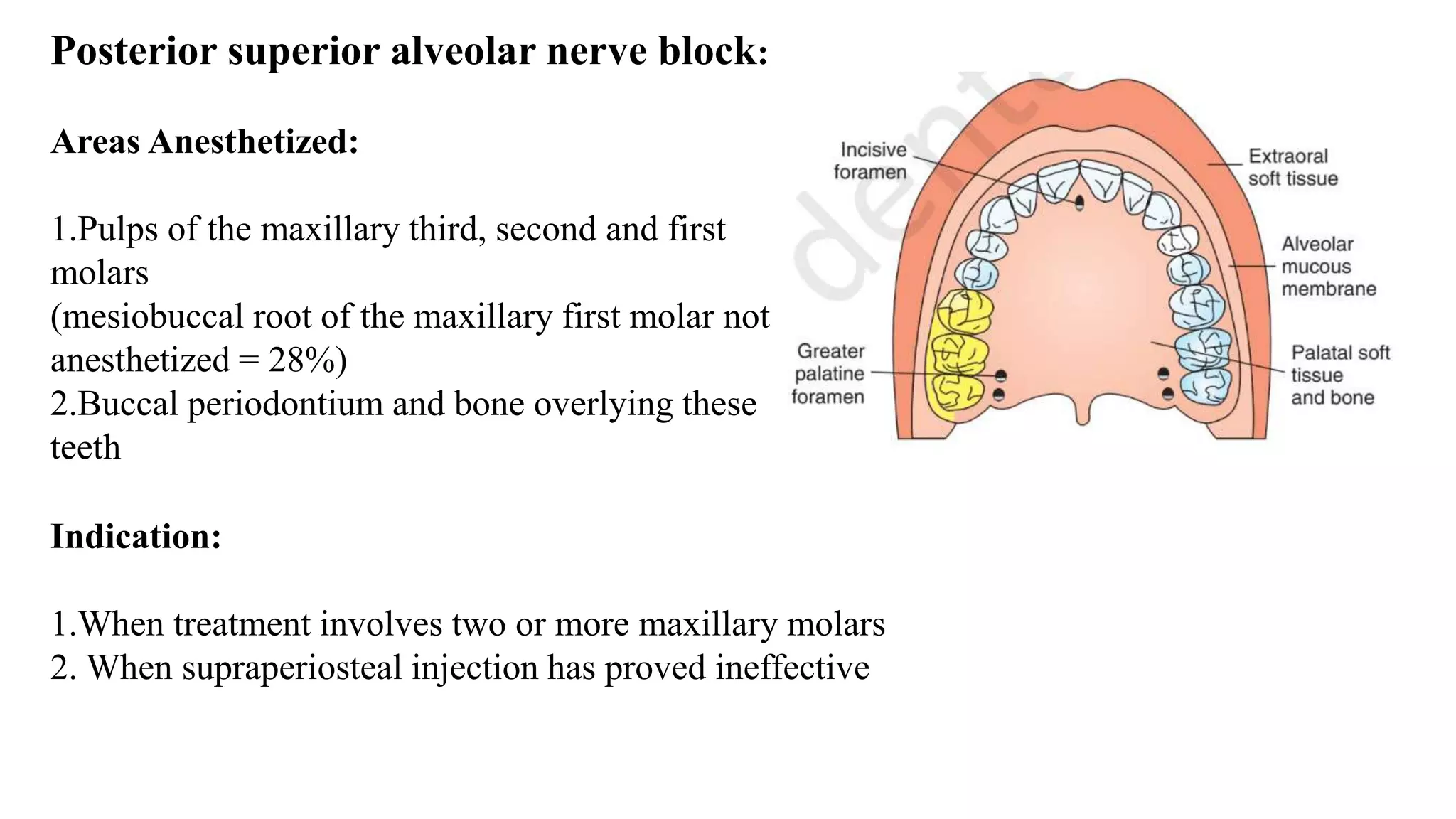













































































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)






