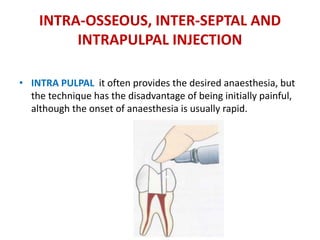
This document provides an overview of local anaesthesia techniques for children. It discusses definitions of local anaesthesia and various techniques including surface anaesthesia, infiltration, nerve blocks, and recent advances. It covers local anaesthetic solutions, pharmacological and non-pharmacological pain control methods, and complications of local anaesthesia such as allergic reactions and toxicity when using local anaesthetics in children. The goal is to provide effective pain control while minimizing risks for paediatric dental procedures.


![SINGLE-TOOTH ANESTHESIA [STA]
• In 2006, the manufacturers of the original CCLAD, introduced a
new device, Single Tooth Anesthesia (STA)
• PRINCIPLE It incorporates dynamic pressure-sensing (DPS)
technology that provides a constant monitoring of the pressure of
local anaesthetic solution during the drug administration.](https://image.slidesharecdn.com/localanaesthesiainchildren-copy-170712090439/85/Local-anaesthesia-for-children-dentistry-38-320.jpg)

![F. DENTIPATCH [INTRAORAL LIGNOCAINE
PATCH]
• Dentipatch contains 10-20% lidocaine, which is
placed on dried mucosa for 15 minutes.
• Disadvantages include central nervous system and
cardiovascular system complications.](https://image.slidesharecdn.com/localanaesthesiainchildren-copy-170712090439/85/Local-anaesthesia-for-children-dentistry-54-320.jpg)










































![Local Anesthesia in childs [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/localanesthesiainchildsautosaved-240712192726-fceb4391-thumbnail.jpg?width=640&height=640&fit=bounds)


























