Downloaded 58 times
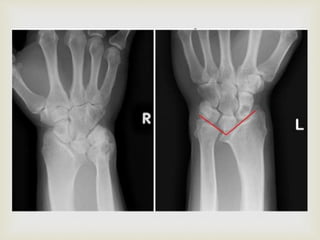
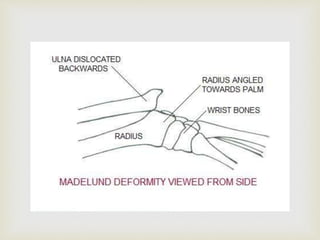


The document discusses Madelung's deformity, an abnormality of the distal radius characterized by ulnar and volar tilt with dorsal subluxation of the ulna. It explores its causes, associations, clinical features, classification, and treatment options, including conservative management and surgical interventions. Notable surgical techniques mentioned include radial osteotomies and excision of the ligament of Vickers, particularly for persistent deformities or pain.





















































































