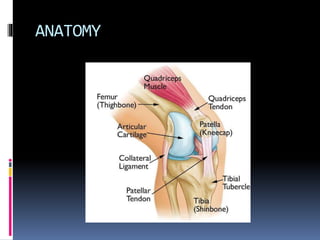
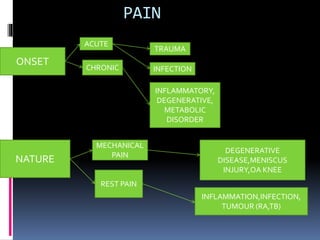
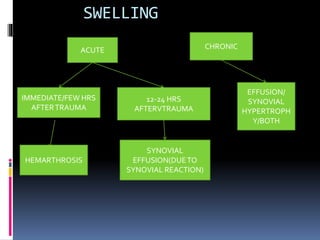
The document summarizes the anatomy and clinical evaluation of the knee joint. It describes the knee as a modified hinge joint composed of the tibiofemoral and patellofemoral joints. Key anatomical structures including the menisci, cruciate ligaments, collateral ligaments, and muscles are outlined. The clinical evaluation involves obtaining a history of pain, swelling, instability, etc and performing an examination involving inspection, palpation, range of motion testing, and special tests of ligaments and menisci.



![MENISCAL TESTS
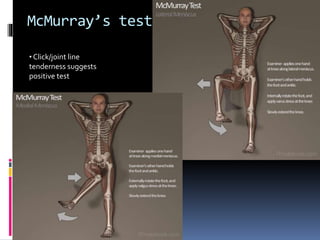
1.McMurray’s test
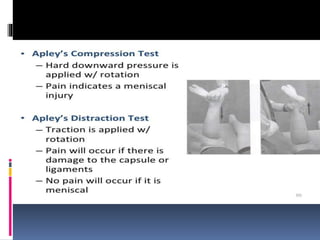
2.Apley’s grinding
test(compression
[meniscus] & distraction
[lig.] ) test
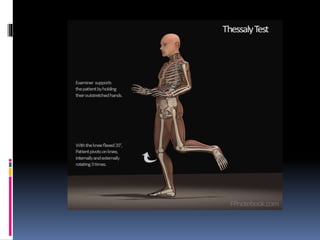
3.Thessaly test: (most
sensitive & specific).](https://image.slidesharecdn.com/kneeexaminationbydryagnik-200202174046/85/Knee-clinical-examination-by-Dr-YAGNIK-34-320.jpg)













































![knee_pres_1[1]](https://cdn.slidesharecdn.com/ss_thumbnails/kneepres11-1272133291-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)






















