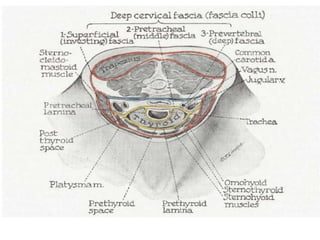
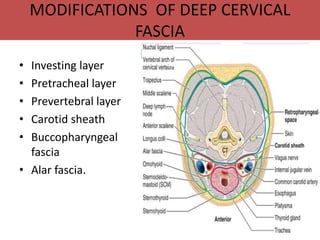
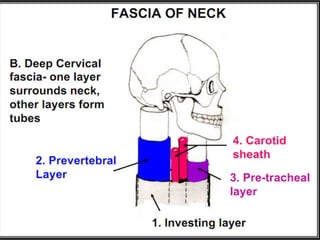
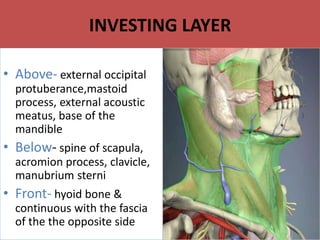
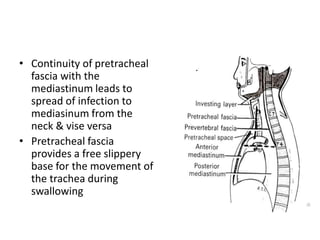
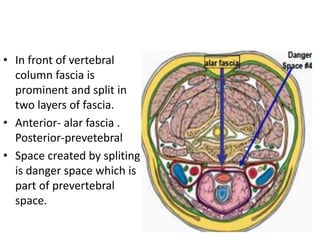
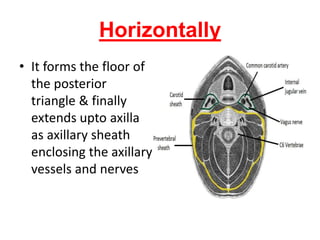
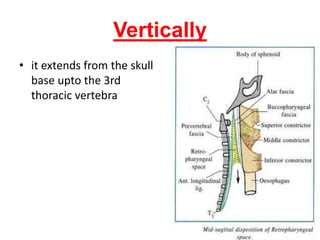
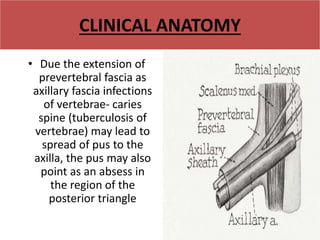
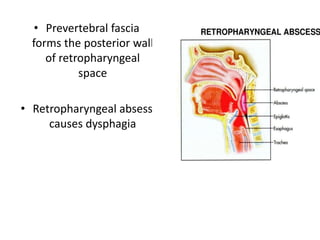
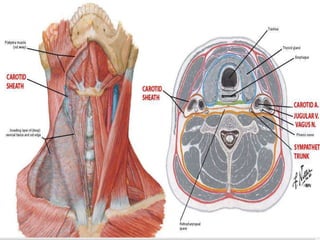
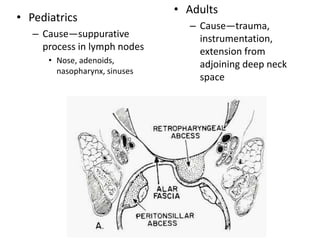
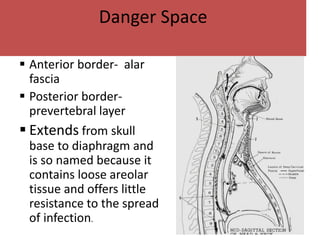
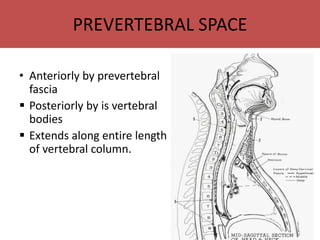
Cervical fascia refers to the fibrous connective tissue in the neck region. There are two types - superficial fascia just below the skin, and deep fascia surrounding muscles, blood vessels and organs in the neck. The deep cervical fascia forms layers around structures like the pretracheal fascia around the trachea and thyroid, and the prevertebral fascia in front of the vertebrae. It also forms sheaths like the carotid sheath containing blood vessels. Infections can potentially spread between neck spaces bounded by these fascial layers, like from the retropharyngeal space to the danger space or prevertebral space. The fascial planes are clinically important for spread of infections and sur