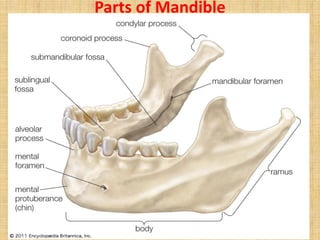
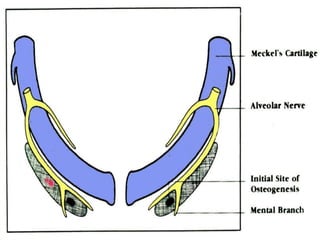
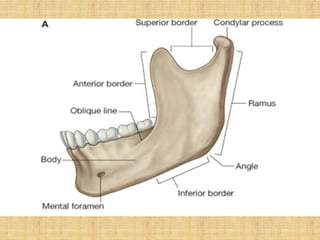
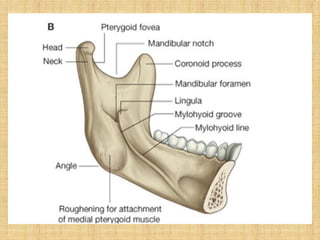
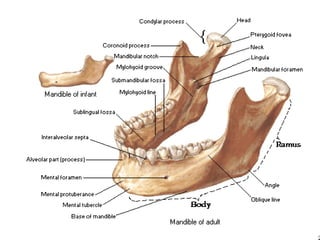
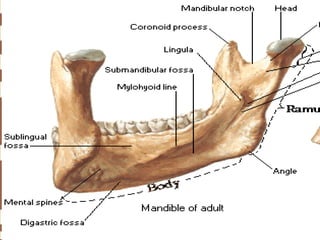
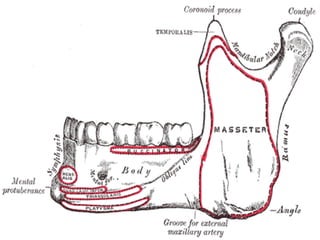
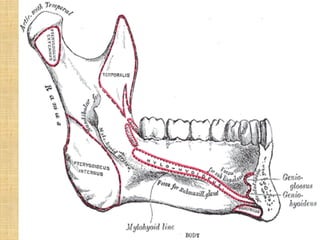
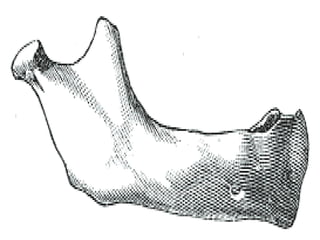
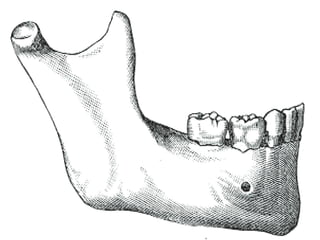
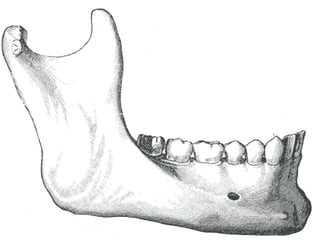
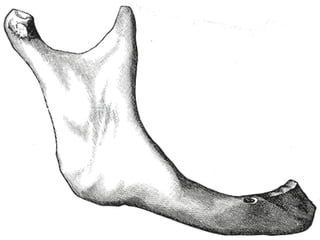
This document provides an overview of the anatomy of the mandible. It discusses the parts and features of the mandible, including the body, ramus, condylar process and coronoid process. It describes the ossification, attachments, blood supply, nerve supply and age-related changes of the mandible. Key points covered include the mandible ossifying from Meckel's cartilage, its attachments to muscles like the masseter and temporalis, the inferior alveolar artery and nerve supplying it, and how its shape changes with age with tooth eruption and absorption.