Downloaded 150 times

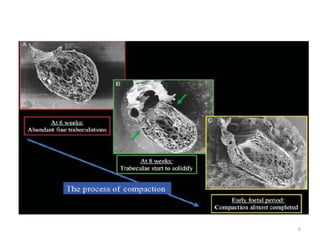


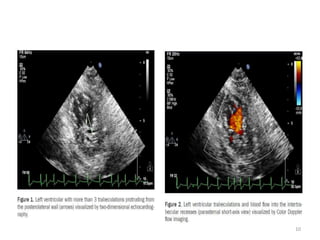
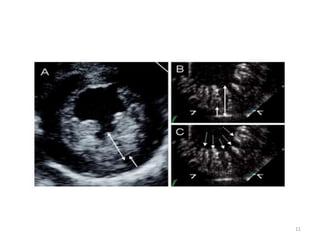
































Left ventricular non-compaction (LVNC) is a rare congenital cardiomyopathy characterized by prominent trabeculations and deep recesses in the left ventricle. Development of LVNC occurs during embryonic myocardial maturation and may vary in severity; diagnostic criteria encompass echocardiographic and cardiac magnetic resonance imaging methods. Management lacks specific treatments, though family screening and genetic testing are recommended, alongside devices for patients with decreased systolic function.























































































