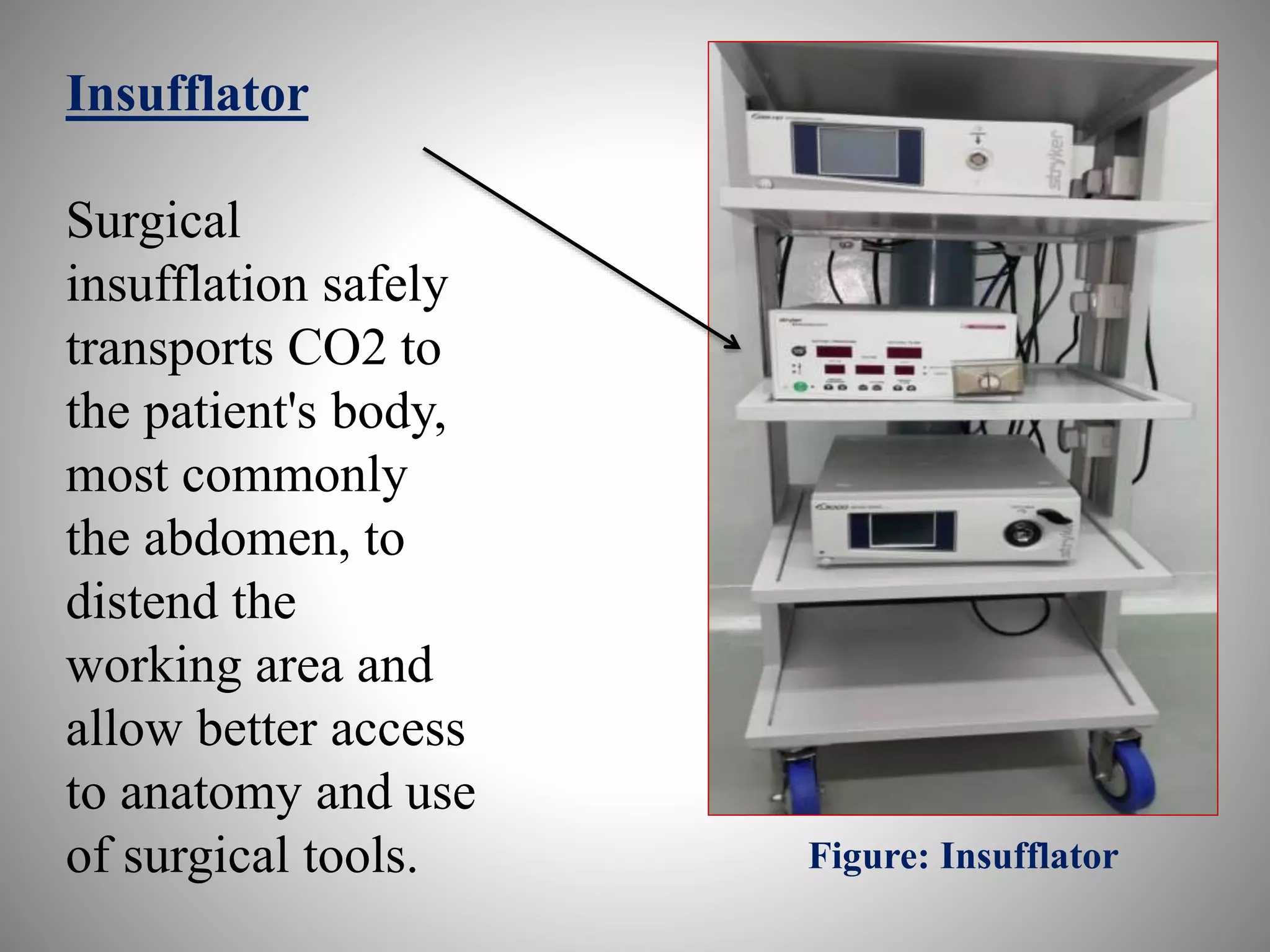
The document provides a comprehensive overview of laparoscopic instruments, including their general description, principles, and components such as the insufflating system, imaging system, and various surgical instruments. Key highlights include the roles of equipment carts, insufflation systems, and surgical monitors, as well as detailed descriptions of essential instruments like trocar, scissors, and needle holders used during laparoscopic procedures. The document aims to educate on the functionality and design considerations essential for performing laparoscopic surgery.