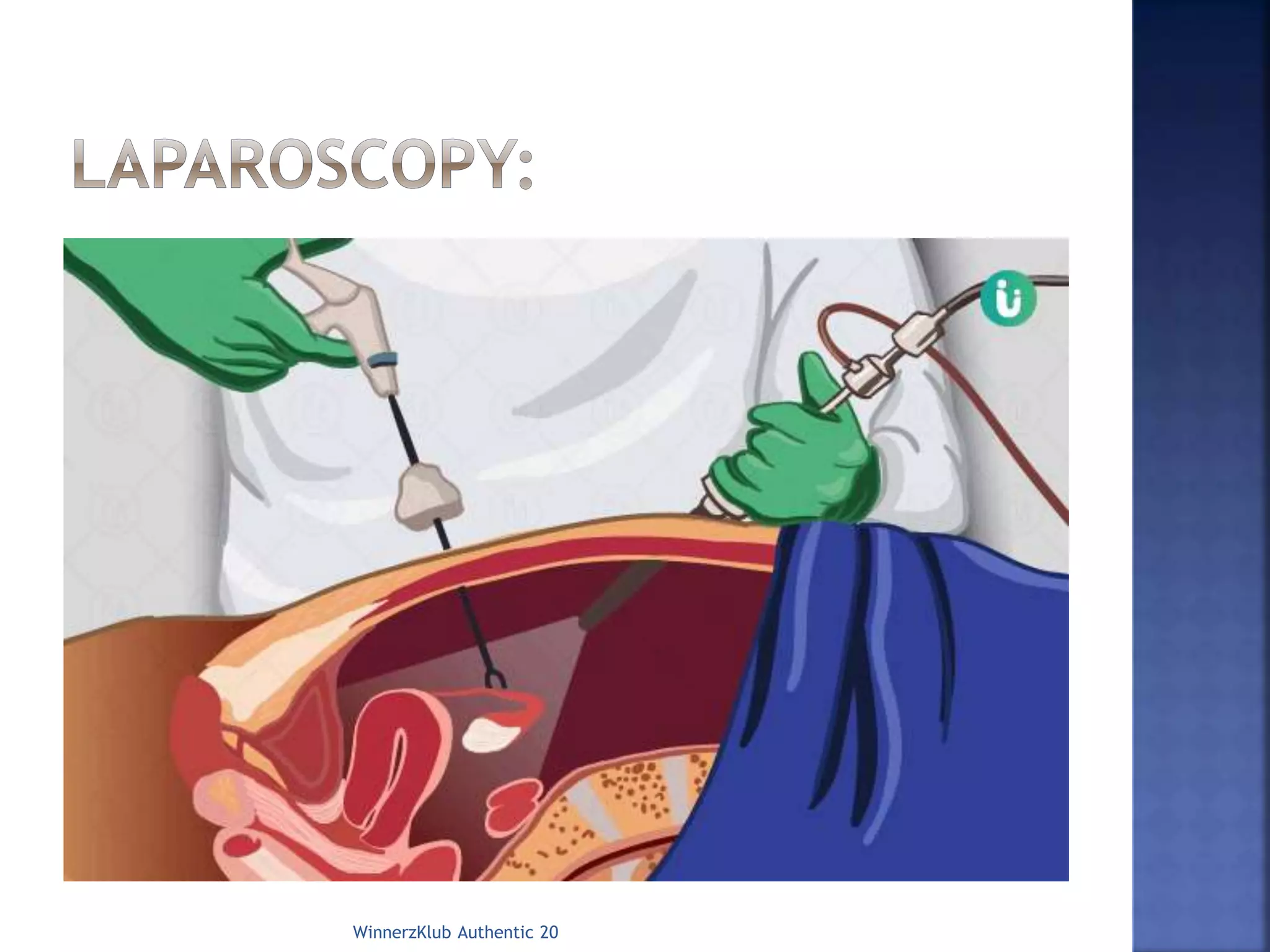
The document discusses laparoscopy, also known as keyhole surgery. It is a minimally invasive surgical procedure that uses small incisions and an instrument called a laparoscope to access the inside of the abdomen without having to make large incisions. The document outlines the indications, advantages, disadvantages, and steps involved in a laparoscopic procedure, including pre-operative preparation, positioning, insertion of trocars, conducting the surgery using instruments, and potential post-operative complications.