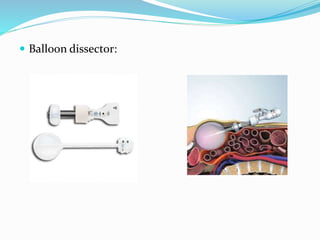
This document provides an overview of laparoscopic instrumentation used in minimally invasive surgery. It discusses the key components needed, including optical devices like telescopes and cameras, equipment for insufflation, trocars and other instruments for accessing the surgical site. A variety of operative instruments are described, such as graspers, dissectors, scissors, and bowel/lung clamps. Energy sources like electrosurgery, ultrasonic devices, and staplers are also covered. The document concludes with a discussion of instruments for tissue approximation and hemostasis, including clip appliers and mechanical staplers, as well as some miscellaneous tools.