Downloaded 10 times












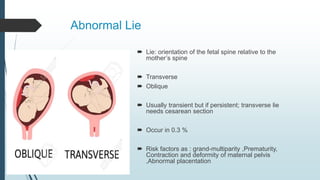








This document discusses abnormal labor, which includes any deviations from normal spontaneous labor of a singleton fetus in cephalic presentation at term. Abnormal labor can occur due to poor progress, fetal compromise, malpresentation, multiple gestation, uterine scar, or induction of labor. Poor progress is defined as less than 2 cm dilation in 4 hours and can be caused by dysfunctional uterine contractions, cephalic-pelvic disproportion, or malpresentation. Malpresentations include abnormal lie, face/brow presentations, breech presentation, and compound presentations. Management depends on identifying the underlying cause based on the 3 Ps - powers (uterine contractions), passages (maternal pelvis), and passenger (fetus).































![ABNORMAL LABOUR[]{}#%^*+=_\|~<>€£¥•.,?!’-/:(($$&@“.,?!’pdf](https://cdn.slidesharecdn.com/ss_thumbnails/abnormallabour-240814080030-7769169f-thumbnail.jpg?width=640&height=640&fit=bounds)























































