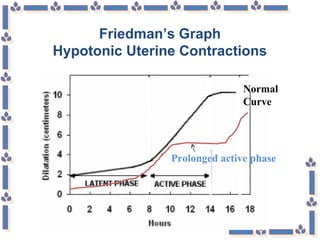
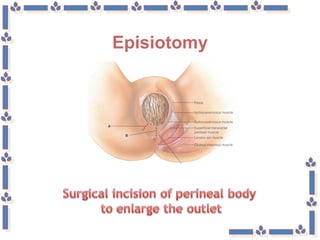
This document discusses various complications that can occur during labor and delivery. It defines dystocia as an abnormal, long, or difficult labor or delivery. It identifies the critical factors that can impact labor as the psyche, powers, passenger, and passageway. It then discusses specific complications like uterine dystocia from large babies or overstretching of the uterus. It provides assessments, treatments, and nursing considerations for complications like hypotonic uterine contractions and prolonged labor. Surgical interventions like forceps delivery, vacuum extraction, episiotomy and cesarean delivery are also outlined.

















































![Abnormal Labor [ Natnael Dechasa Gemeda pdf ].pdf](https://cdn.slidesharecdn.com/ss_thumbnails/abnormallabornatnaeldechasagemedapdf-230317103358-a4021124-thumbnail.jpg?width=640&height=640&fit=bounds)








































