Download to read offline


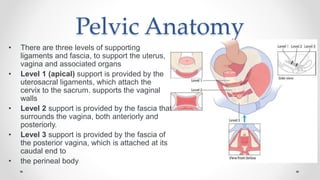












Uterovaginal prolapse is caused by failure of pelvic floor muscles and ligaments to support pelvic organs. Symptoms include a sensation of vaginal bulge or protrusion, as well as pain and discomfort relieved by lying down. Pelvic organs are supported by three levels of ligaments and fascia, with defects at different levels causing prolapse of different organs. Clinical assessment involves examination of the prolapse severity and other symptoms. Management includes pelvic floor exercises, pessaries, and surgery depending on the severity and patient preferences.



































































