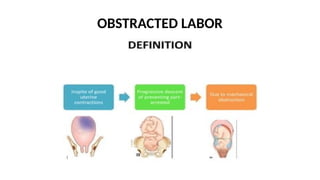
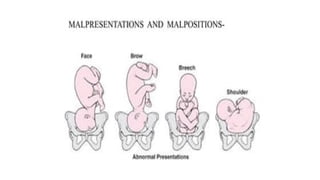
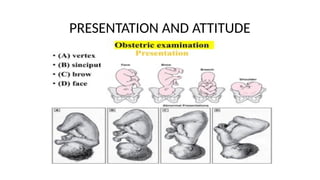
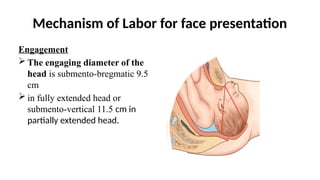
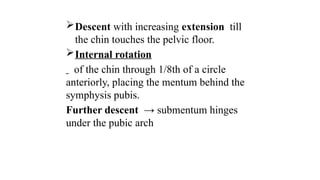
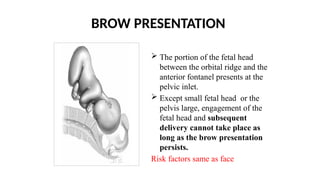
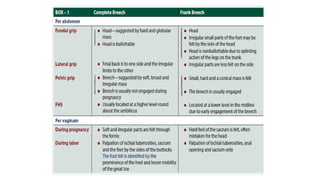
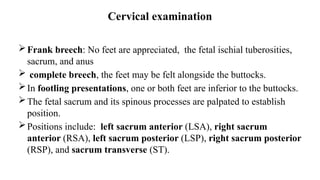
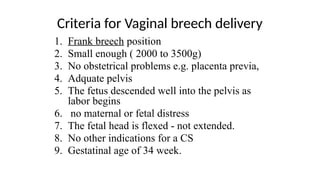
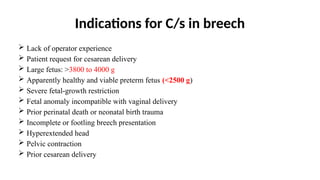
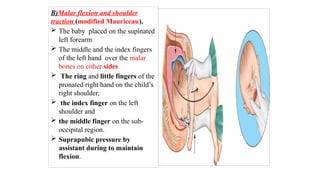
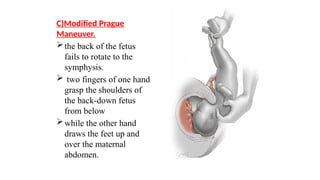
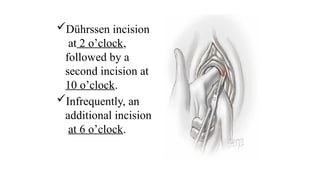
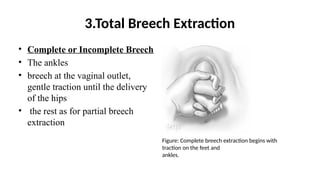
The document discusses obstructed labor, highlighting its various causes, including bony and soft tissue obstructions, as well as fetal malpositions. It delves into clinical features, complications for both mother and fetus, and preventive measures, emphasizing the importance of antenatal detection and timely intervention. The document also outlines management strategies for various malpresentations like face and breech presentations, discussing their definitions, diagnosis, and management approaches.