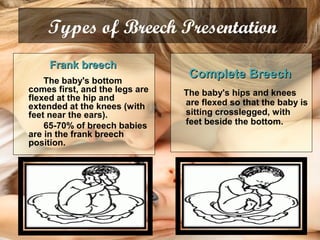
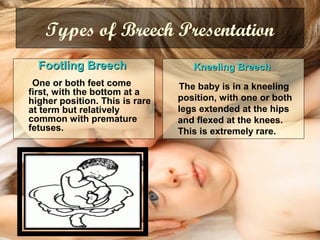
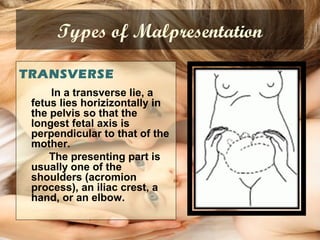
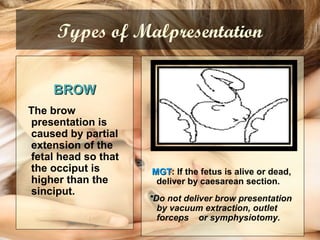
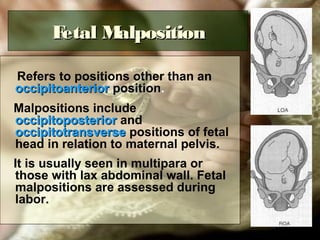
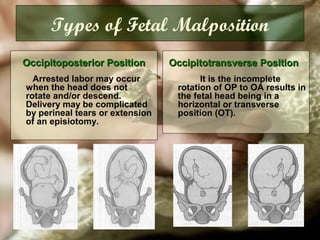
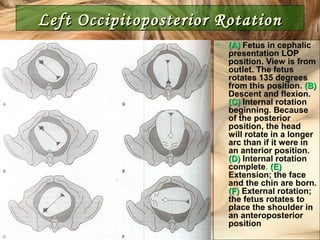
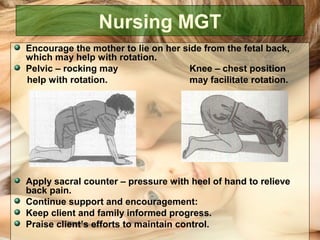
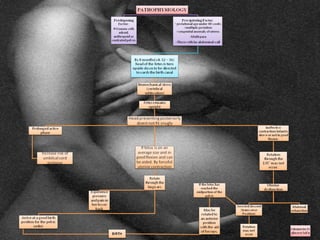
This document discusses fetal malpresentation and malposition. It defines malpresentation as the fetal presenting part being something other than vertex, such as breech, transverse, face or brow. Malposition refers to positions other than occipitoanterior, such as occipitoposterior or occipitotransverse. It describes the different types of breech, transverse, face and brow presentations. It discusses the risks of malpresentation/malposition to both mother and fetus. It provides guidelines for managing different malpresentations/malpositions which may include external cephalic version, vaginal delivery, forceps delivery, vacuum extraction, caesarean section or symphysiotomy. It emphasizes the importance of monitoring labor